{"title":"用左心房应变预测接受体外循环冠状动脉旁路移植术患者的术后心房颤动","authors":"Deepak Prakash Borde MD, DNB, FCA, FTEE , Shreedhar Joshi MD, FCA, DM, FTEE , Ashish Agrawal DNB (Surg), MCh , Deepak Bhavsar MS, MCh , Pooja Joshi MD, FIACTA, FTEE , Pramod Apsingkar MD, DPM","doi":"10.1053/j.jvca.2024.07.047","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Postoperative atrial fibrillation (POAF) is associated with increased morbidity, mortality, and length of hospital stay. The objective of this study was to assess the utility of left atrial strain (LAS) to predict POAF in patients undergoing off-pump coronary artery bypass grafting (OPCABG).</div></div><div><h3>Design</h3><div>Retrospective observational study.</div></div><div><h3>Setting</h3><div>Tertiary care hospital.</div></div><div><h3>Participants</h3><div>103 patients undergoing OPCABG.</div></div><div><h3>Interventions</h3><div>None.</div></div><div><h3>Measurements and Results</h3><div>In addition to comprehensive transthoracic echocardiography, LAS was measured for reservoir (R), conduction (CD), and contraction (CT) components. POAF was defined as new electrocardiographic evidence of AF requiring treatment. Logistic regression was done to assess factors associated with POAF. The diagnostic accuracy of variables in predicting POAF was assessed by receiver operating characteristic analysis. POAF was documented in 24 (23.3%) patients. There was no difference in ejection fraction, average global longitudinal strain, or proportion of left ventricular diastolic dysfunction grades between patients with POAF and patients without POAF. All three components of LAS: LAS R (19.2 ± 4.7 <em>v</em> 23.5 ± 4.8, p < 0.001), LAS CD (8.9 ± 3.7 <em>v</em> 12.3 ± 4.8, p = 0.1), and LAS CT (10.3 ± 3.9 <em>v</em> 12.1 ± 4.1, p = 0.04), were significantly lower among patients with POAF compared with patients without POAF, respectively. According to univariate analysis, all components of LAS were statistically significant predictors of POAF. In multivariate analysis, only age (odds ratio = 1.08, p = 0.025) and LAS R (odds ratio = 0.84, p = 0.004) were independently associated with POAF. LAS R was a better predictor of POAF, with an area under the curve (AUC) of 0.758, than LAS CD (AUC = 0.67) and LAS CT (AUC = 0.62). LAS R had an optimal cutoff of 23% with sensitivity of 95.8% (confidence interval: 78.9-99.9%) and specificity of 49.4% (37.9-60.9%) to predict POAF.</div></div><div><h3>Conclusions</h3><div>LAS R is a significant predictor of POAF, and its use can be recommended for screening of OPCABG patients at high risk of POAF.</div></div>","PeriodicalId":15176,"journal":{"name":"Journal of cardiothoracic and vascular anesthesia","volume":"38 11","pages":"Pages 2582-2591"},"PeriodicalIF":2.1000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Left Atrial Strain to Predict Postoperative Atrial Fibrillation in Patients Undergoing Off-pump Coronary Artery Bypass Graft\",\"authors\":\"Deepak Prakash Borde MD, DNB, FCA, FTEE , Shreedhar Joshi MD, FCA, DM, FTEE , Ashish Agrawal DNB (Surg), MCh , Deepak Bhavsar MS, MCh , Pooja Joshi MD, FIACTA, FTEE , Pramod Apsingkar MD, DPM\",\"doi\":\"10.1053/j.jvca.2024.07.047\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><div>Postoperative atrial fibrillation (POAF) is associated with increased morbidity, mortality, and length of hospital stay. The objective of this study was to assess the utility of left atrial strain (LAS) to predict POAF in patients undergoing off-pump coronary artery bypass grafting (OPCABG).</div></div><div><h3>Design</h3><div>Retrospective observational study.</div></div><div><h3>Setting</h3><div>Tertiary care hospital.</div></div><div><h3>Participants</h3><div>103 patients undergoing OPCABG.</div></div><div><h3>Interventions</h3><div>None.</div></div><div><h3>Measurements and Results</h3><div>In addition to comprehensive transthoracic echocardiography, LAS was measured for reservoir (R), conduction (CD), and contraction (CT) components. POAF was defined as new electrocardiographic evidence of AF requiring treatment. Logistic regression was done to assess factors associated with POAF. The diagnostic accuracy of variables in predicting POAF was assessed by receiver operating characteristic analysis. POAF was documented in 24 (23.3%) patients. There was no difference in ejection fraction, average global longitudinal strain, or proportion of left ventricular diastolic dysfunction grades between patients with POAF and patients without POAF. All three components of LAS: LAS R (19.2 ± 4.7 <em>v</em> 23.5 ± 4.8, p < 0.001), LAS CD (8.9 ± 3.7 <em>v</em> 12.3 ± 4.8, p = 0.1), and LAS CT (10.3 ± 3.9 <em>v</em> 12.1 ± 4.1, p = 0.04), were significantly lower among patients with POAF compared with patients without POAF, respectively. According to univariate analysis, all components of LAS were statistically significant predictors of POAF. In multivariate analysis, only age (odds ratio = 1.08, p = 0.025) and LAS R (odds ratio = 0.84, p = 0.004) were independently associated with POAF. LAS R was a better predictor of POAF, with an area under the curve (AUC) of 0.758, than LAS CD (AUC = 0.67) and LAS CT (AUC = 0.62). LAS R had an optimal cutoff of 23% with sensitivity of 95.8% (confidence interval: 78.9-99.9%) and specificity of 49.4% (37.9-60.9%) to predict POAF.</div></div><div><h3>Conclusions</h3><div>LAS R is a significant predictor of POAF, and its use can be recommended for screening of OPCABG patients at high risk of POAF.</div></div>\",\"PeriodicalId\":15176,\"journal\":{\"name\":\"Journal of cardiothoracic and vascular anesthesia\",\"volume\":\"38 11\",\"pages\":\"Pages 2582-2591\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cardiothoracic and vascular anesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1053077024005081\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cardiothoracic and vascular anesthesia","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1053077024005081","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:术后心房颤动(POAF)与发病率、死亡率和住院时间的增加有关。本研究旨在评估左心房应变(LAS)在预测接受体外循环冠状动脉旁路移植术(OPCABG)患者术后心房颤动的实用性:设计:回顾性观察研究:参与者: 103名接受OPCABG手术的患者干预措施:无:测量和结果除了全面的经胸超声心动图外,还测量了 LAS 的储能(R)、传导(CD)和收缩(CT)成分。POAF定义为需要治疗的房颤新心电图证据。采用逻辑回归评估与 POAF 相关的因素。通过接收器操作特征分析评估了预测 POAF 变量的诊断准确性。有 24 例(23.3%)患者被记录为 POAF。在射血分数、平均整体纵向应变或左心室舒张功能障碍等级比例方面,POAF 患者与非 POAF 患者之间没有差异。LAS的所有三个组成部分:LAS R(19.2 ± 4.7 v 23.5 ± 4.8,p < 0.001)、LAS CD(8.9 ± 3.7 v 12.3 ± 4.8,p = 0.1)和LAS CT(10.3 ± 3.9 v 12.1 ± 4.1,p = 0.04)在POAF患者中分别明显低于非POAF患者。根据单变量分析,LAS 的所有组成部分均可在统计学上显著预测 POAF。在多变量分析中,只有年龄(几率比=1.08,P=0.025)和 LAS R(几率比=0.84,P=0.004)与 POAF 独立相关。与 LAS CD(AUC = 0.67)和 LAS CT(AUC = 0.62)相比,LAS R 能更好地预测 POAF,其曲线下面积(AUC)为 0.758。LAS R的最佳临界值为23%,预测POAF的灵敏度为95.8%(置信区间:78.9-99.9%),特异度为49.4%(37.9-60.9%):LAS R 是预测 POAF 的重要指标,建议用于筛查 POAF 高风险的 OPCABG 患者。
Left Atrial Strain to Predict Postoperative Atrial Fibrillation in Patients Undergoing Off-pump Coronary Artery Bypass Graft
Objective
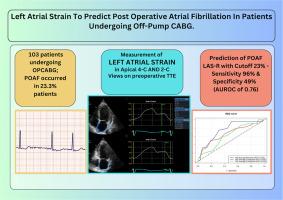
Postoperative atrial fibrillation (POAF) is associated with increased morbidity, mortality, and length of hospital stay. The objective of this study was to assess the utility of left atrial strain (LAS) to predict POAF in patients undergoing off-pump coronary artery bypass grafting (OPCABG).
Design
Retrospective observational study.
Setting
Tertiary care hospital.
Participants
103 patients undergoing OPCABG.
Interventions
None.
Measurements and Results
In addition to comprehensive transthoracic echocardiography, LAS was measured for reservoir (R), conduction (CD), and contraction (CT) components. POAF was defined as new electrocardiographic evidence of AF requiring treatment. Logistic regression was done to assess factors associated with POAF. The diagnostic accuracy of variables in predicting POAF was assessed by receiver operating characteristic analysis. POAF was documented in 24 (23.3%) patients. There was no difference in ejection fraction, average global longitudinal strain, or proportion of left ventricular diastolic dysfunction grades between patients with POAF and patients without POAF. All three components of LAS: LAS R (19.2 ± 4.7 v 23.5 ± 4.8, p < 0.001), LAS CD (8.9 ± 3.7 v 12.3 ± 4.8, p = 0.1), and LAS CT (10.3 ± 3.9 v 12.1 ± 4.1, p = 0.04), were significantly lower among patients with POAF compared with patients without POAF, respectively. According to univariate analysis, all components of LAS were statistically significant predictors of POAF. In multivariate analysis, only age (odds ratio = 1.08, p = 0.025) and LAS R (odds ratio = 0.84, p = 0.004) were independently associated with POAF. LAS R was a better predictor of POAF, with an area under the curve (AUC) of 0.758, than LAS CD (AUC = 0.67) and LAS CT (AUC = 0.62). LAS R had an optimal cutoff of 23% with sensitivity of 95.8% (confidence interval: 78.9-99.9%) and specificity of 49.4% (37.9-60.9%) to predict POAF.
Conclusions
LAS R is a significant predictor of POAF, and its use can be recommended for screening of OPCABG patients at high risk of POAF.
期刊介绍:
The Journal of Cardiothoracic and Vascular Anesthesia is primarily aimed at anesthesiologists who deal with patients undergoing cardiac, thoracic or vascular surgical procedures. JCVA features a multidisciplinary approach, with contributions from cardiac, vascular and thoracic surgeons, cardiologists, and other related specialists. Emphasis is placed on rapid publication of clinically relevant material.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
