Emese Zsarnoczay, Nicola Fink, U Joseph Schoepf, Daniel Pinos, Jim O'Doherty, Thomas Allmendinger, Junia Hagenauer, Joseph P Griffith Iii, Milán Vecsey-Nagy, Pál Maurovich-Horvat, Tilman Emrich, Akos Varga-Szemes
{"title":"用光子计数 CT 评估血管狭窄的超高分辨率和虚拟无钙重建算法的准确性:动态模型研究的结果。","authors":"Emese Zsarnoczay, Nicola Fink, U Joseph Schoepf, Daniel Pinos, Jim O'Doherty, Thomas Allmendinger, Junia Hagenauer, Joseph P Griffith Iii, Milán Vecsey-Nagy, Pál Maurovich-Horvat, Tilman Emrich, Akos Varga-Szemes","doi":"10.1186/s41747-024-00482-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We compared ultra-high resolution (UHR), standard resolution (SR), and virtual non-calcium (VNCa) reconstruction for coronary artery stenosis evaluation using photon-counting computed tomography (PC-CT).</p><p><strong>Methods: </strong>One vessel phantom (4-mm diameter) containing solid calcified lesions with 25% and 50% stenoses inside a thorax phantom with motion simulation underwent PC-CT using UHR (0.2-mm slice thickness) and SR (0.6-mm slice thickness) at heart rates of 60 beats per minute (bpm), 80 bpm, and 100 bpm. A paired t-test or Wilcoxon test with Bonferroni correction was used.</p><p><strong>Results: </strong>For 50% stenosis, differences in percent mean diameter stenosis between UHR and SR at 60 bpm (51.0 vs 60.3), 80 bpm (51.7 vs 59.6), and 100 bpm (53.7 vs 59.0) (p ≤ 0.011), as well as between VNCa and SR at 60 bpm (50.6 vs 60.3), 80 bpm (51.5 vs 59.6), and 100 bpm (53.7 vs 59.0) were significant (p ≤ 0.011), while differences between UHR and VNCa at all heart rates (p ≥ 0.327) were not significant. For 25% stenosis, differences between UHR and SR at 60 bpm (28.0 vs 33.7), 80 bpm (28.4 vs 34.3), and VNCa vs SR at 60 bpm (29.1 vs 33.7) were significant (p ≤ 0.015), while differences for UHR vs SR at 100 bpm (29.9 vs 34.0), as well as for VNCa vs SR at 80 bpm (30.7 vs 34.3) and 100 bpm (33.1 vs 34.0) were not significant (p ≥ 0.028).</p><p><strong>Conclusion: </strong>Stenosis quantification accuracy with PC-CT improved using either UHR acquisition or VNCa reconstruction.</p><p><strong>Relevance statement: </strong>PC-CT offers to scan with UHR mode and the reconstruction of VNCa images both of them could provide improved coronary stenosis quantification at increased heart rates, allowing a more accurate stenosis grading at low and high heart rates compared to SR.</p><p><strong>Key points: </strong>Evaluation of coronary stenosis with conventional CT is challenging at high heart rates. PC-CT allows for scanning with ECG-gated UHR and SR modes. UHR and VNCa images were compared in a dynamic phantom. UHR improves stenosis quantification up to 100 bpm. VNCa reconstruction improves stenosis evaluation up to 80 bpm.</p>","PeriodicalId":36926,"journal":{"name":"European Radiology Experimental","volume":"8 1","pages":"102"},"PeriodicalIF":3.6000,"publicationDate":"2024-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362394/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of ultra-high resolution and virtual non-calcium reconstruction algorithm for stenosis evaluation with photon-counting CT: results from a dynamic phantom study.\",\"authors\":\"Emese Zsarnoczay, Nicola Fink, U Joseph Schoepf, Daniel Pinos, Jim O'Doherty, Thomas Allmendinger, Junia Hagenauer, Joseph P Griffith Iii, Milán Vecsey-Nagy, Pál Maurovich-Horvat, Tilman Emrich, Akos Varga-Szemes\",\"doi\":\"10.1186/s41747-024-00482-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We compared ultra-high resolution (UHR), standard resolution (SR), and virtual non-calcium (VNCa) reconstruction for coronary artery stenosis evaluation using photon-counting computed tomography (PC-CT).</p><p><strong>Methods: </strong>One vessel phantom (4-mm diameter) containing solid calcified lesions with 25% and 50% stenoses inside a thorax phantom with motion simulation underwent PC-CT using UHR (0.2-mm slice thickness) and SR (0.6-mm slice thickness) at heart rates of 60 beats per minute (bpm), 80 bpm, and 100 bpm. A paired t-test or Wilcoxon test with Bonferroni correction was used.</p><p><strong>Results: </strong>For 50% stenosis, differences in percent mean diameter stenosis between UHR and SR at 60 bpm (51.0 vs 60.3), 80 bpm (51.7 vs 59.6), and 100 bpm (53.7 vs 59.0) (p ≤ 0.011), as well as between VNCa and SR at 60 bpm (50.6 vs 60.3), 80 bpm (51.5 vs 59.6), and 100 bpm (53.7 vs 59.0) were significant (p ≤ 0.011), while differences between UHR and VNCa at all heart rates (p ≥ 0.327) were not significant. For 25% stenosis, differences between UHR and SR at 60 bpm (28.0 vs 33.7), 80 bpm (28.4 vs 34.3), and VNCa vs SR at 60 bpm (29.1 vs 33.7) were significant (p ≤ 0.015), while differences for UHR vs SR at 100 bpm (29.9 vs 34.0), as well as for VNCa vs SR at 80 bpm (30.7 vs 34.3) and 100 bpm (33.1 vs 34.0) were not significant (p ≥ 0.028).</p><p><strong>Conclusion: </strong>Stenosis quantification accuracy with PC-CT improved using either UHR acquisition or VNCa reconstruction.</p><p><strong>Relevance statement: </strong>PC-CT offers to scan with UHR mode and the reconstruction of VNCa images both of them could provide improved coronary stenosis quantification at increased heart rates, allowing a more accurate stenosis grading at low and high heart rates compared to SR.</p><p><strong>Key points: </strong>Evaluation of coronary stenosis with conventional CT is challenging at high heart rates. PC-CT allows for scanning with ECG-gated UHR and SR modes. UHR and VNCa images were compared in a dynamic phantom. UHR improves stenosis quantification up to 100 bpm. VNCa reconstruction improves stenosis evaluation up to 80 bpm.</p>\",\"PeriodicalId\":36926,\"journal\":{\"name\":\"European Radiology Experimental\",\"volume\":\"8 1\",\"pages\":\"102\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362394/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Radiology Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41747-024-00482-w\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Radiology Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41747-024-00482-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:我们比较了使用光子计数计算机断层扫描(PC-CT)进行冠状动脉狭窄评估的超高分辨率(UHR)、标准分辨率(SR)和虚拟无钙(VNCa)重建:方法:在一个具有运动模拟功能的胸腔模型中,使用 UHR(0.2 毫米切片厚度)和 SR(0.6 毫米切片厚度),在心率为每分钟 60 次、80 次和 100 次的条件下,对一个含有 25% 和 50% 狭窄实心钙化病变的血管模型(直径为 4 毫米)进行 PC-CT。采用配对 t 检验或带有 Bonferroni 校正的 Wilcoxon 检验:结果:对于 50%的狭窄,UHR 和 SR 在 60 bpm(51.0 vs 60.3)、80 bpm(51.7 vs 59.6)和 100 bpm(53.7 vs 59.0)时的平均直径狭窄百分比差异(p ≤ 0.011),以及 VNCa 和 SR 在 60 bpm(50.6 vs 60.3)、80 bpm(51.7 vs 59.6)和 100 bpm(53.7 vs 59.0)时的平均直径狭窄百分比差异(p ≤ 0.011)。6 vs 60.3)、80 bpm(51.5 vs 59.6)和 100 bpm(53.7 vs 59.0)时 VNCa 和 SR 之间的差异显著(p ≤ 0.011),而 UHR 和 VNCa 在所有心率下的差异均不显著(p ≥ 0.327)。对于 25% 的狭窄,UHR 与 SR 在 60 bpm(28.0 vs 33.7)、80 bpm(28.4 vs 34.3)以及 VNCa 与 SR 在 60 bpm(29.1 vs 33.7)时的差异均有显著性(p ≤ 0.015),而 100 bpm 时 UHR vs SR(29.9 vs 34.0)以及 80 bpm 时 VNCa vs SR(30.7 vs 34.3)和 100 bpm 时 VNCa vs SR(33.1 vs 34.0)的差异不显著(P ≥ 0.028):结论:使用 UHR 采集或 VNCa 重建,PC-CT 的狭窄量化准确性有所提高:PC-CT提供UHR模式扫描和VNCa图像重建,两者都能在心率增加时改善冠状动脉狭窄的量化,与SR相比,在低心率和高心率时能更准确地进行狭窄分级:要点:使用传统 CT 评估冠状动脉狭窄在高心率下具有挑战性。PC-CT 允许使用心电图门控的 UHR 和 SR 模式进行扫描。在动态模型中比较了 UHR 和 VNCa 图像。UHR 可改善血管狭窄的量化,最高可达 100 bpm。VNCa 重建可改善血管狭窄评估,最高可达 80 bpm。
Accuracy of ultra-high resolution and virtual non-calcium reconstruction algorithm for stenosis evaluation with photon-counting CT: results from a dynamic phantom study.
Background: We compared ultra-high resolution (UHR), standard resolution (SR), and virtual non-calcium (VNCa) reconstruction for coronary artery stenosis evaluation using photon-counting computed tomography (PC-CT).
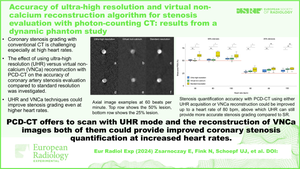
Methods: One vessel phantom (4-mm diameter) containing solid calcified lesions with 25% and 50% stenoses inside a thorax phantom with motion simulation underwent PC-CT using UHR (0.2-mm slice thickness) and SR (0.6-mm slice thickness) at heart rates of 60 beats per minute (bpm), 80 bpm, and 100 bpm. A paired t-test or Wilcoxon test with Bonferroni correction was used.
Results: For 50% stenosis, differences in percent mean diameter stenosis between UHR and SR at 60 bpm (51.0 vs 60.3), 80 bpm (51.7 vs 59.6), and 100 bpm (53.7 vs 59.0) (p ≤ 0.011), as well as between VNCa and SR at 60 bpm (50.6 vs 60.3), 80 bpm (51.5 vs 59.6), and 100 bpm (53.7 vs 59.0) were significant (p ≤ 0.011), while differences between UHR and VNCa at all heart rates (p ≥ 0.327) were not significant. For 25% stenosis, differences between UHR and SR at 60 bpm (28.0 vs 33.7), 80 bpm (28.4 vs 34.3), and VNCa vs SR at 60 bpm (29.1 vs 33.7) were significant (p ≤ 0.015), while differences for UHR vs SR at 100 bpm (29.9 vs 34.0), as well as for VNCa vs SR at 80 bpm (30.7 vs 34.3) and 100 bpm (33.1 vs 34.0) were not significant (p ≥ 0.028).
Conclusion: Stenosis quantification accuracy with PC-CT improved using either UHR acquisition or VNCa reconstruction.
Relevance statement: PC-CT offers to scan with UHR mode and the reconstruction of VNCa images both of them could provide improved coronary stenosis quantification at increased heart rates, allowing a more accurate stenosis grading at low and high heart rates compared to SR.
Key points: Evaluation of coronary stenosis with conventional CT is challenging at high heart rates. PC-CT allows for scanning with ECG-gated UHR and SR modes. UHR and VNCa images were compared in a dynamic phantom. UHR improves stenosis quantification up to 100 bpm. VNCa reconstruction improves stenosis evaluation up to 80 bpm.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
