Quincy K Tran, Anastasia Ternovskaia, Jessica V Downing, Minahil Cheema, Taylor Kowansky, Isha Vashee, Jasjot Sayal, Jasmine Wu, Aditi Singh, Daniel J Haase
{"title":"重症监护复苏室对农村患者获得四级护理的影响:比较分析。","authors":"Quincy K Tran, Anastasia Ternovskaia, Jessica V Downing, Minahil Cheema, Taylor Kowansky, Isha Vashee, Jasjot Sayal, Jasmine Wu, Aditi Singh, Daniel J Haase","doi":"10.1155/2024/9599855","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous research suggests that patients from rural areas who are critically ill with complex medical needs or require time-sensitive subspecialty interventions face worse healthcare outcomes and delays in care when compared to those from urban areas. The critical care resuscitation unit (CCRU) at our quaternary care center was established to expedite the transfer of critically ill patients or those who need time-sensitive intervention. This study investigates if disparities exist in treatments and outcomes among patients transferred to the CCRU from rural versus urban hospitals.</p><p><strong>Methods: </strong>This is a retrospective study of adult, nontrauma patients admitted to the CCRU via interhospital transfer from outside facilities from January 1 to December 31, 2018. Patients transferred from within our institution or with missing clinical data were excluded. Multivariable logistic regressions were performed to measure the association between patients' demographic and clinical factors with in-hospital mortality.</p><p><strong>Results: </strong>We analyzed 1381 nontrauma patients, and 484 (35%) were from rural areas. Median age was 59 [47-69], and 629 (46%) were female. Median sequential organ failure assessment was 3 ([1-6], <i>p</i>=0.062) for both patients transferred from urban and rural hospitals. There was no significant difference between groups with respect to most demographic and clinical factors, as well as types of interventions after CCRU arrival, including emergent surgical interventions within 12 hours of arrival at the CCRU. Rural patients were more likely to be transferred for care by the acute care emergency surgery service than were patients from urban areas and were transferred over a significantly greater distance (difference of 53 kilometers (km), 95% CI: -58.9-51.7 km, <i>P</i> < 0.001). Transfer from rural areas was not associated with increased odds of in-hospital mortality (OR: 0.90, 95% CI: 0.60, 1.36; <i>P</i>=0.63).</p><p><strong>Conclusion: </strong>Thirty-five percent of patients transferred to the CCRU came from rural areas, which house 25% of the state population of Maryland. Patients transferred from rural counties to the CCRU faced greater transport distances, but they received the same level of care upon arrival at the CCRU and had the same odds of in-hospital mortality as patients transferred from urban hospitals.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2024 ","pages":"9599855"},"PeriodicalIF":1.8000,"publicationDate":"2024-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362575/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of the Critical Care Resuscitation Unit on Quaternary Care Accessibility for Rural Patients: A Comparative Analysis.\",\"authors\":\"Quincy K Tran, Anastasia Ternovskaia, Jessica V Downing, Minahil Cheema, Taylor Kowansky, Isha Vashee, Jasjot Sayal, Jasmine Wu, Aditi Singh, Daniel J Haase\",\"doi\":\"10.1155/2024/9599855\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Previous research suggests that patients from rural areas who are critically ill with complex medical needs or require time-sensitive subspecialty interventions face worse healthcare outcomes and delays in care when compared to those from urban areas. The critical care resuscitation unit (CCRU) at our quaternary care center was established to expedite the transfer of critically ill patients or those who need time-sensitive intervention. This study investigates if disparities exist in treatments and outcomes among patients transferred to the CCRU from rural versus urban hospitals.</p><p><strong>Methods: </strong>This is a retrospective study of adult, nontrauma patients admitted to the CCRU via interhospital transfer from outside facilities from January 1 to December 31, 2018. Patients transferred from within our institution or with missing clinical data were excluded. Multivariable logistic regressions were performed to measure the association between patients' demographic and clinical factors with in-hospital mortality.</p><p><strong>Results: </strong>We analyzed 1381 nontrauma patients, and 484 (35%) were from rural areas. Median age was 59 [47-69], and 629 (46%) were female. Median sequential organ failure assessment was 3 ([1-6], <i>p</i>=0.062) for both patients transferred from urban and rural hospitals. There was no significant difference between groups with respect to most demographic and clinical factors, as well as types of interventions after CCRU arrival, including emergent surgical interventions within 12 hours of arrival at the CCRU. Rural patients were more likely to be transferred for care by the acute care emergency surgery service than were patients from urban areas and were transferred over a significantly greater distance (difference of 53 kilometers (km), 95% CI: -58.9-51.7 km, <i>P</i> < 0.001). Transfer from rural areas was not associated with increased odds of in-hospital mortality (OR: 0.90, 95% CI: 0.60, 1.36; <i>P</i>=0.63).</p><p><strong>Conclusion: </strong>Thirty-five percent of patients transferred to the CCRU came from rural areas, which house 25% of the state population of Maryland. Patients transferred from rural counties to the CCRU faced greater transport distances, but they received the same level of care upon arrival at the CCRU and had the same odds of in-hospital mortality as patients transferred from urban hospitals.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2024 \",\"pages\":\"9599855\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11362575/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/9599855\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/9599855","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
The Impact of the Critical Care Resuscitation Unit on Quaternary Care Accessibility for Rural Patients: A Comparative Analysis.
Background: Previous research suggests that patients from rural areas who are critically ill with complex medical needs or require time-sensitive subspecialty interventions face worse healthcare outcomes and delays in care when compared to those from urban areas. The critical care resuscitation unit (CCRU) at our quaternary care center was established to expedite the transfer of critically ill patients or those who need time-sensitive intervention. This study investigates if disparities exist in treatments and outcomes among patients transferred to the CCRU from rural versus urban hospitals.
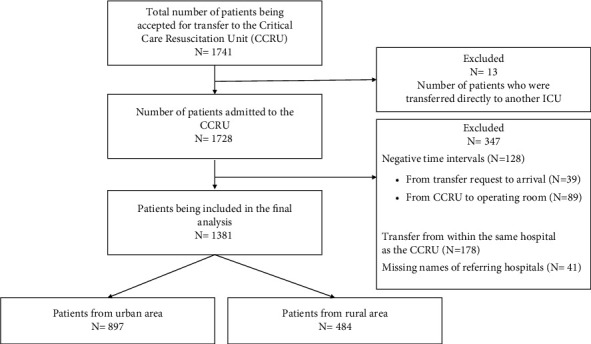
Methods: This is a retrospective study of adult, nontrauma patients admitted to the CCRU via interhospital transfer from outside facilities from January 1 to December 31, 2018. Patients transferred from within our institution or with missing clinical data were excluded. Multivariable logistic regressions were performed to measure the association between patients' demographic and clinical factors with in-hospital mortality.
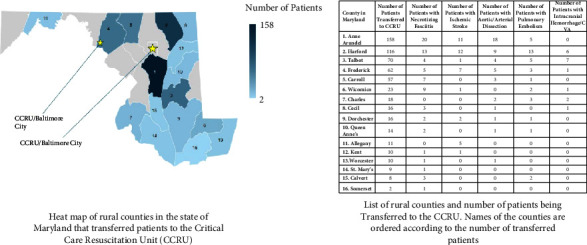
Results: We analyzed 1381 nontrauma patients, and 484 (35%) were from rural areas. Median age was 59 [47-69], and 629 (46%) were female. Median sequential organ failure assessment was 3 ([1-6], p=0.062) for both patients transferred from urban and rural hospitals. There was no significant difference between groups with respect to most demographic and clinical factors, as well as types of interventions after CCRU arrival, including emergent surgical interventions within 12 hours of arrival at the CCRU. Rural patients were more likely to be transferred for care by the acute care emergency surgery service than were patients from urban areas and were transferred over a significantly greater distance (difference of 53 kilometers (km), 95% CI: -58.9-51.7 km, P < 0.001). Transfer from rural areas was not associated with increased odds of in-hospital mortality (OR: 0.90, 95% CI: 0.60, 1.36; P=0.63).
Conclusion: Thirty-five percent of patients transferred to the CCRU came from rural areas, which house 25% of the state population of Maryland. Patients transferred from rural counties to the CCRU faced greater transport distances, but they received the same level of care upon arrival at the CCRU and had the same odds of in-hospital mortality as patients transferred from urban hospitals.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
