Mohsen Sadatsafavi , Amir Khakban , Tima Mohammadi , Samir Gupta , Nick Bansback , the IMPACT Study Team
{"title":"由利益相关者提供信息的疾病标志物和风险评分阳性阈值:方法框架及在阻塞性肺病中的应用。","authors":"Mohsen Sadatsafavi , Amir Khakban , Tima Mohammadi , Samir Gupta , Nick Bansback , the IMPACT Study Team","doi":"10.1016/j.jclinepi.2024.111509","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>A positivity threshold is often applied to markers or predicted risks to guide disease management. These thresholds are often decided exclusively by clinical experts despite being sensitive to the preferences of patients and general public as ultimate stakeholders.</div></div><div><h3>Study Design and Setting</h3><div>We propose an analytical framework for quantifying the net benefit (NB) of an evidence-based positivity threshold based on combining preference-sensitive (eg, how individuals weight benefits and harms of treatment) and preference-agnostic (eg, the magnitude of benefit and the risk of harm) parameters. We propose parsimonious choice experiments to elicit preference-sensitive parameters from stakeholders, and targeted evidence synthesis to quantify the value of preference-agnostic parameters. We apply this framework to maintenance of azithromycin therapy for chronic obstructive pulmonary disease using a discrete choice experiment to estimate preference weights for attribute level associated with treatment. We identify the positivity threshold on 12-month moderate or severe exacerbation risk that would maximize the NB of treatment in terms of severe exacerbations avoided.</div></div><div><h3>Results</h3><div>In the case study, the prevention of moderate and severe exacerbations (benefits) and the risk of hearing loss and gastrointestinal symptoms (harms) emerged as important attributes. Four hundred seventy seven respondents completed the discrete choice experiment survey. Relative to each percent risk of severe exacerbation, preference weights for each percent risk of moderate exacerbation, hearing loss, and gastrointestinal symptoms were 0.395 (95% confidence interval [CI] 0.338–0.456), 1.180 (95% CI 1.071–1.201), and 0.253 (95% CI 0.207–0.299), respectively. The optimal threshold that maximized NB was to treat patients with a 12-month risk of moderate or severe exacerbations ≥12%.</div></div><div><h3>Conclusion</h3><div>The proposed methodology can be applied to many contexts where the objective is to devise positivity thresholds that need to incorporate stakeholder preferences. Applying this framework to chronic obstructive pulmonary disease pharmacotherapy resulted in a stakeholder-informed treatment threshold that was substantially lower than the implicit thresholds in contemporary guidelines.</div></div><div><h3>Plain Language Summary</h3><div>Doctors often compare disease markers (such as laboratory results) or risk scores for a patient with cut-off values from guidelines to decide which patients need to be treated. For example, guidelines recommend that patients whose 10-year risk of heart attack is more than 10% be given statin pills. However, guidelines that recommend such treatment rules might not consider what matters most to patients (like how much they do not like side effects of the drugs). In this study, we propose a mathematical method where preferences of individuals on the trade-off between treatment benefits and harms can be used to determine the best treatment rule. We apply this method to the choice of antibiotic therapy for patients with lung airway diseases. We find that, given patient and public preferences on treatment benefit and risks, those with a 12% or more risk of experiencing a lung attack should receive antibiotic therapy. This patient-oriented cut-off is significantly lower than the cut-off values currently used by guidelines, which are in the 60%–70% range. We recommend applying this method whenever scientists must make recommendations on treatment rules where patient or public preferences might influence those rules.</div></div>","PeriodicalId":51079,"journal":{"name":"Journal of Clinical Epidemiology","volume":"175 ","pages":"Article 111509"},"PeriodicalIF":5.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0895435624002658/pdfft?md5=338502f05fab7320074c3310f0f3dcac&pid=1-s2.0-S0895435624002658-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Stakeholder-informed positivity thresholds for disease markers and risk scores: a methodological framework and an application in obstructive lung disease\",\"authors\":\"Mohsen Sadatsafavi , Amir Khakban , Tima Mohammadi , Samir Gupta , Nick Bansback , the IMPACT Study Team\",\"doi\":\"10.1016/j.jclinepi.2024.111509\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><div>A positivity threshold is often applied to markers or predicted risks to guide disease management. These thresholds are often decided exclusively by clinical experts despite being sensitive to the preferences of patients and general public as ultimate stakeholders.</div></div><div><h3>Study Design and Setting</h3><div>We propose an analytical framework for quantifying the net benefit (NB) of an evidence-based positivity threshold based on combining preference-sensitive (eg, how individuals weight benefits and harms of treatment) and preference-agnostic (eg, the magnitude of benefit and the risk of harm) parameters. We propose parsimonious choice experiments to elicit preference-sensitive parameters from stakeholders, and targeted evidence synthesis to quantify the value of preference-agnostic parameters. We apply this framework to maintenance of azithromycin therapy for chronic obstructive pulmonary disease using a discrete choice experiment to estimate preference weights for attribute level associated with treatment. We identify the positivity threshold on 12-month moderate or severe exacerbation risk that would maximize the NB of treatment in terms of severe exacerbations avoided.</div></div><div><h3>Results</h3><div>In the case study, the prevention of moderate and severe exacerbations (benefits) and the risk of hearing loss and gastrointestinal symptoms (harms) emerged as important attributes. Four hundred seventy seven respondents completed the discrete choice experiment survey. Relative to each percent risk of severe exacerbation, preference weights for each percent risk of moderate exacerbation, hearing loss, and gastrointestinal symptoms were 0.395 (95% confidence interval [CI] 0.338–0.456), 1.180 (95% CI 1.071–1.201), and 0.253 (95% CI 0.207–0.299), respectively. The optimal threshold that maximized NB was to treat patients with a 12-month risk of moderate or severe exacerbations ≥12%.</div></div><div><h3>Conclusion</h3><div>The proposed methodology can be applied to many contexts where the objective is to devise positivity thresholds that need to incorporate stakeholder preferences. Applying this framework to chronic obstructive pulmonary disease pharmacotherapy resulted in a stakeholder-informed treatment threshold that was substantially lower than the implicit thresholds in contemporary guidelines.</div></div><div><h3>Plain Language Summary</h3><div>Doctors often compare disease markers (such as laboratory results) or risk scores for a patient with cut-off values from guidelines to decide which patients need to be treated. For example, guidelines recommend that patients whose 10-year risk of heart attack is more than 10% be given statin pills. However, guidelines that recommend such treatment rules might not consider what matters most to patients (like how much they do not like side effects of the drugs). In this study, we propose a mathematical method where preferences of individuals on the trade-off between treatment benefits and harms can be used to determine the best treatment rule. We apply this method to the choice of antibiotic therapy for patients with lung airway diseases. We find that, given patient and public preferences on treatment benefit and risks, those with a 12% or more risk of experiencing a lung attack should receive antibiotic therapy. This patient-oriented cut-off is significantly lower than the cut-off values currently used by guidelines, which are in the 60%–70% range. We recommend applying this method whenever scientists must make recommendations on treatment rules where patient or public preferences might influence those rules.</div></div>\",\"PeriodicalId\":51079,\"journal\":{\"name\":\"Journal of Clinical Epidemiology\",\"volume\":\"175 \",\"pages\":\"Article 111509\"},\"PeriodicalIF\":5.2000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0895435624002658/pdfft?md5=338502f05fab7320074c3310f0f3dcac&pid=1-s2.0-S0895435624002658-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0895435624002658\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/8/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0895435624002658","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Stakeholder-informed positivity thresholds for disease markers and risk scores: a methodological framework and an application in obstructive lung disease
Objectives
A positivity threshold is often applied to markers or predicted risks to guide disease management. These thresholds are often decided exclusively by clinical experts despite being sensitive to the preferences of patients and general public as ultimate stakeholders.
Study Design and Setting
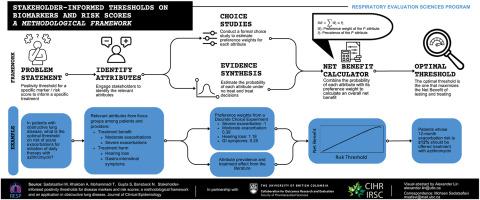
We propose an analytical framework for quantifying the net benefit (NB) of an evidence-based positivity threshold based on combining preference-sensitive (eg, how individuals weight benefits and harms of treatment) and preference-agnostic (eg, the magnitude of benefit and the risk of harm) parameters. We propose parsimonious choice experiments to elicit preference-sensitive parameters from stakeholders, and targeted evidence synthesis to quantify the value of preference-agnostic parameters. We apply this framework to maintenance of azithromycin therapy for chronic obstructive pulmonary disease using a discrete choice experiment to estimate preference weights for attribute level associated with treatment. We identify the positivity threshold on 12-month moderate or severe exacerbation risk that would maximize the NB of treatment in terms of severe exacerbations avoided.
Results
In the case study, the prevention of moderate and severe exacerbations (benefits) and the risk of hearing loss and gastrointestinal symptoms (harms) emerged as important attributes. Four hundred seventy seven respondents completed the discrete choice experiment survey. Relative to each percent risk of severe exacerbation, preference weights for each percent risk of moderate exacerbation, hearing loss, and gastrointestinal symptoms were 0.395 (95% confidence interval [CI] 0.338–0.456), 1.180 (95% CI 1.071–1.201), and 0.253 (95% CI 0.207–0.299), respectively. The optimal threshold that maximized NB was to treat patients with a 12-month risk of moderate or severe exacerbations ≥12%.
Conclusion
The proposed methodology can be applied to many contexts where the objective is to devise positivity thresholds that need to incorporate stakeholder preferences. Applying this framework to chronic obstructive pulmonary disease pharmacotherapy resulted in a stakeholder-informed treatment threshold that was substantially lower than the implicit thresholds in contemporary guidelines.
Plain Language Summary
Doctors often compare disease markers (such as laboratory results) or risk scores for a patient with cut-off values from guidelines to decide which patients need to be treated. For example, guidelines recommend that patients whose 10-year risk of heart attack is more than 10% be given statin pills. However, guidelines that recommend such treatment rules might not consider what matters most to patients (like how much they do not like side effects of the drugs). In this study, we propose a mathematical method where preferences of individuals on the trade-off between treatment benefits and harms can be used to determine the best treatment rule. We apply this method to the choice of antibiotic therapy for patients with lung airway diseases. We find that, given patient and public preferences on treatment benefit and risks, those with a 12% or more risk of experiencing a lung attack should receive antibiotic therapy. This patient-oriented cut-off is significantly lower than the cut-off values currently used by guidelines, which are in the 60%–70% range. We recommend applying this method whenever scientists must make recommendations on treatment rules where patient or public preferences might influence those rules.
期刊介绍:
The Journal of Clinical Epidemiology strives to enhance the quality of clinical and patient-oriented healthcare research by advancing and applying innovative methods in conducting, presenting, synthesizing, disseminating, and translating research results into optimal clinical practice. Special emphasis is placed on training new generations of scientists and clinical practice leaders.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
