Maria I Rodriguez, Thomas H A Meath, Ashley Daly, Kelsey Watson, K John McConnell, Hyunjee Kim
{"title":"十二个月避孕药具供应政策和医疗补助避孕药具配发。","authors":"Maria I Rodriguez, Thomas H A Meath, Ashley Daly, Kelsey Watson, K John McConnell, Hyunjee Kim","doi":"10.1001/jamahealthforum.2024.2755","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Nineteen states have passed legislation requiring insurers to cover the dispensation of a 12-month supply of short-acting, hormonal contraception.</p><p><strong>Objective: </strong>To determine whether 12-month contraceptive supply policies were associated with an increase in the receipt of 12-month or longer supply of contraception.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study included data from all female Medicaid enrollees aged 18 to 44 years who used short-acting hormonal contraception (ie, pill, patch, or ring) from 2016 to 2020.</p><p><strong>Exposures: </strong>Eleven treatment states where legislation required insurers to cover a 12-month supply of contraception to continuing users and 25 comparison states without such legislation prior to December 2020.</p><p><strong>Main outcomes and measures: </strong>Proportion of contraception months received via a single 12-month or longer fill.</p><p><strong>Results: </strong>This study included 48 255 512 months of dispensed oral pill, patch, and ring contraception prescription supply among 4 778 264 female Medicaid enrollees. The majority of months of supplied contraception were for the contraceptive pill rather than the patch or ring. In a staggered difference-in-differences model, the 12-month supply policy was associated with an estimated 4.39-percentage point (pp) increase (95% CI, 4.38 pp-4.40 pp) in the proportion of contraception dispensed as part of a 12-month or longer supply, from a mean of 0.11% in treatment states during the first quarter of the study period. Investigating the heterogeneity in policy association across states, California stood out with a 7.17-pp increase (95% CI, 7.15 pp-7.19 pp) in the proportion of contraception dispensed as a 12-month or longer supply; in the other 10 treatment states, the policy association was less than 1 pp.</p><p><strong>Conclusions and relevance: </strong>In this cohort study of Medicaid recipients using short-acting hormonal contraception, the passage of a 12-month contraceptive supply policy was associated with a minimal increase in the proportion of contraception dispensed through a 12-month or longer supply.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"5 8","pages":"e242755"},"PeriodicalIF":11.3000,"publicationDate":"2024-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364992/pdf/","citationCount":"0","resultStr":"{\"title\":\"Twelve-Month Contraceptive Supply Policies and Medicaid Contraceptive Dispensing.\",\"authors\":\"Maria I Rodriguez, Thomas H A Meath, Ashley Daly, Kelsey Watson, K John McConnell, Hyunjee Kim\",\"doi\":\"10.1001/jamahealthforum.2024.2755\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Nineteen states have passed legislation requiring insurers to cover the dispensation of a 12-month supply of short-acting, hormonal contraception.</p><p><strong>Objective: </strong>To determine whether 12-month contraceptive supply policies were associated with an increase in the receipt of 12-month or longer supply of contraception.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study included data from all female Medicaid enrollees aged 18 to 44 years who used short-acting hormonal contraception (ie, pill, patch, or ring) from 2016 to 2020.</p><p><strong>Exposures: </strong>Eleven treatment states where legislation required insurers to cover a 12-month supply of contraception to continuing users and 25 comparison states without such legislation prior to December 2020.</p><p><strong>Main outcomes and measures: </strong>Proportion of contraception months received via a single 12-month or longer fill.</p><p><strong>Results: </strong>This study included 48 255 512 months of dispensed oral pill, patch, and ring contraception prescription supply among 4 778 264 female Medicaid enrollees. The majority of months of supplied contraception were for the contraceptive pill rather than the patch or ring. In a staggered difference-in-differences model, the 12-month supply policy was associated with an estimated 4.39-percentage point (pp) increase (95% CI, 4.38 pp-4.40 pp) in the proportion of contraception dispensed as part of a 12-month or longer supply, from a mean of 0.11% in treatment states during the first quarter of the study period. Investigating the heterogeneity in policy association across states, California stood out with a 7.17-pp increase (95% CI, 7.15 pp-7.19 pp) in the proportion of contraception dispensed as a 12-month or longer supply; in the other 10 treatment states, the policy association was less than 1 pp.</p><p><strong>Conclusions and relevance: </strong>In this cohort study of Medicaid recipients using short-acting hormonal contraception, the passage of a 12-month contraceptive supply policy was associated with a minimal increase in the proportion of contraception dispensed through a 12-month or longer supply.</p>\",\"PeriodicalId\":53180,\"journal\":{\"name\":\"JAMA Health Forum\",\"volume\":\"5 8\",\"pages\":\"e242755\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2024-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11364992/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Health Forum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1001/jamahealthforum.2024.2755\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2024.2755","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Twelve-Month Contraceptive Supply Policies and Medicaid Contraceptive Dispensing.
Importance: Nineteen states have passed legislation requiring insurers to cover the dispensation of a 12-month supply of short-acting, hormonal contraception.
Objective: To determine whether 12-month contraceptive supply policies were associated with an increase in the receipt of 12-month or longer supply of contraception.
Design, setting, and participants: This retrospective cohort study included data from all female Medicaid enrollees aged 18 to 44 years who used short-acting hormonal contraception (ie, pill, patch, or ring) from 2016 to 2020.
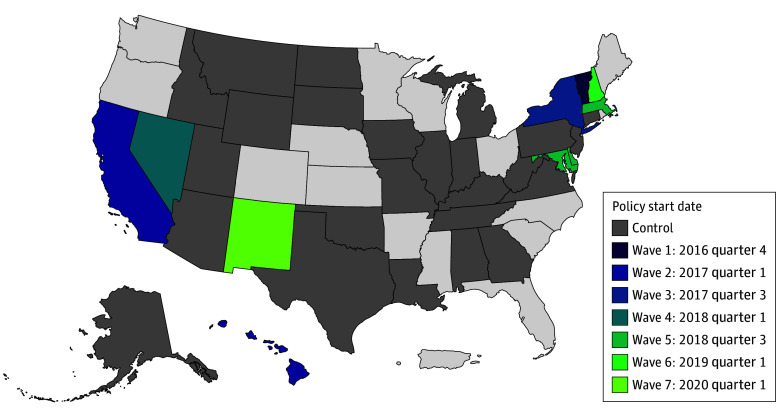
Exposures: Eleven treatment states where legislation required insurers to cover a 12-month supply of contraception to continuing users and 25 comparison states without such legislation prior to December 2020.
Main outcomes and measures: Proportion of contraception months received via a single 12-month or longer fill.
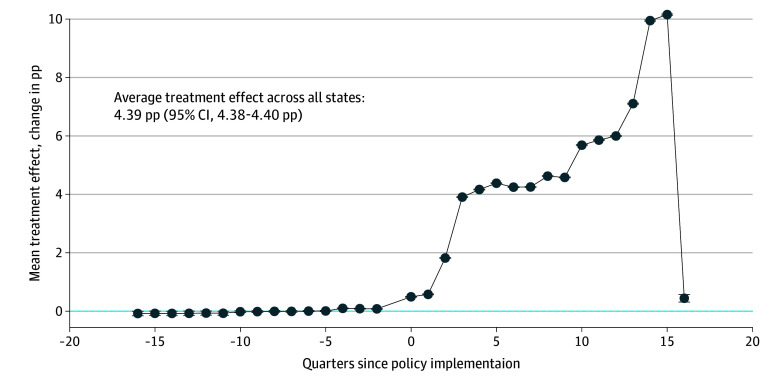
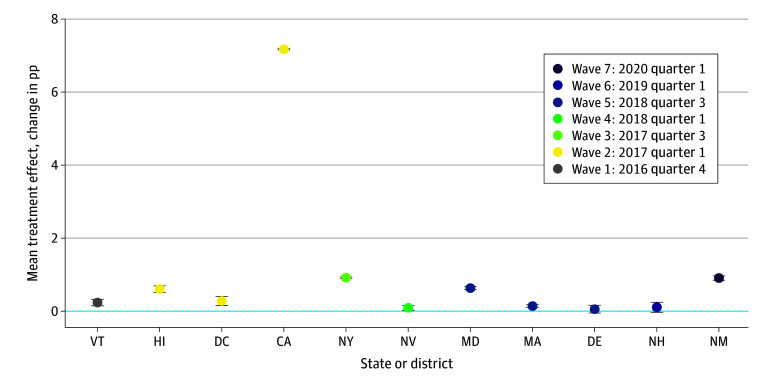
Results: This study included 48 255 512 months of dispensed oral pill, patch, and ring contraception prescription supply among 4 778 264 female Medicaid enrollees. The majority of months of supplied contraception were for the contraceptive pill rather than the patch or ring. In a staggered difference-in-differences model, the 12-month supply policy was associated with an estimated 4.39-percentage point (pp) increase (95% CI, 4.38 pp-4.40 pp) in the proportion of contraception dispensed as part of a 12-month or longer supply, from a mean of 0.11% in treatment states during the first quarter of the study period. Investigating the heterogeneity in policy association across states, California stood out with a 7.17-pp increase (95% CI, 7.15 pp-7.19 pp) in the proportion of contraception dispensed as a 12-month or longer supply; in the other 10 treatment states, the policy association was less than 1 pp.
Conclusions and relevance: In this cohort study of Medicaid recipients using short-acting hormonal contraception, the passage of a 12-month contraceptive supply policy was associated with a minimal increase in the proportion of contraception dispensed through a 12-month or longer supply.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
