Stig Holm Ovesen, Søren Helbo Skaarup, Rasmus Aagaard, Hans Kirkegaard, Bo Løfgren, Michael Dan Arvig, Bo Martin Bibby, Stefan Posth, Christian B Laursen, Jesper Weile
{"title":"护理点超声与标准诊断路径对急诊科呼吸困难患者 24 小时住院时间的影响--随机对照试验方案。","authors":"Stig Holm Ovesen, Søren Helbo Skaarup, Rasmus Aagaard, Hans Kirkegaard, Bo Løfgren, Michael Dan Arvig, Bo Martin Bibby, Stefan Posth, Christian B Laursen, Jesper Weile","doi":"10.2147/OAEM.S454062","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Point-of-care ultrasound (POCUS) helps emergency department (ED) physicians make prompt and appropriate decisions, but the optimal diagnostic integration and potential clinical benefits remain unclear. We describe the protocol and statistical analysis plan for a randomized controlled trial. The objective is to determine the effect of a POCUS-driven diagnostic pathway in adult dyspneic ED patients on the proportion of patients having a hospital stay of less than 24 hours when compared to the standard diagnostic pathway.</p><p><strong>Patients and methods: </strong>This is a multicenter, randomized, investigator-initiated, open-labeled, pragmatic, controlled trial. Adult ED patients with chief complaint dyspnea are eligible. Patients are randomized (1:1) to the POCUS-driven diagnostic pathway or standard diagnostic pathway, with 337 patients in each group. The primary outcome is the proportion of patients having a hospital stay (from ED arrival to hospital discharge) of less than 24 hours. Key secondary outcomes include hospital length-of-stay, 72-hour revisits, and 30-day hospital-free days.</p><p><strong>Conclusion: </strong>Sparse evidence exists for any clinical benefit from a POCUS-integrated diagnostic pathway. The results from this trial will help clarify the promising signals for POCUS to influence patient care among ED patients with dyspnea.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"211-219"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365495/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of a Point-of-Care Ultrasound-Driven vs Standard Diagnostic Pathway on 24-Hour Hospital Stay in Emergency Department Patients with Dyspnea-Protocol for A Randomized Controlled Trial.\",\"authors\":\"Stig Holm Ovesen, Søren Helbo Skaarup, Rasmus Aagaard, Hans Kirkegaard, Bo Løfgren, Michael Dan Arvig, Bo Martin Bibby, Stefan Posth, Christian B Laursen, Jesper Weile\",\"doi\":\"10.2147/OAEM.S454062\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Point-of-care ultrasound (POCUS) helps emergency department (ED) physicians make prompt and appropriate decisions, but the optimal diagnostic integration and potential clinical benefits remain unclear. We describe the protocol and statistical analysis plan for a randomized controlled trial. The objective is to determine the effect of a POCUS-driven diagnostic pathway in adult dyspneic ED patients on the proportion of patients having a hospital stay of less than 24 hours when compared to the standard diagnostic pathway.</p><p><strong>Patients and methods: </strong>This is a multicenter, randomized, investigator-initiated, open-labeled, pragmatic, controlled trial. Adult ED patients with chief complaint dyspnea are eligible. Patients are randomized (1:1) to the POCUS-driven diagnostic pathway or standard diagnostic pathway, with 337 patients in each group. The primary outcome is the proportion of patients having a hospital stay (from ED arrival to hospital discharge) of less than 24 hours. Key secondary outcomes include hospital length-of-stay, 72-hour revisits, and 30-day hospital-free days.</p><p><strong>Conclusion: </strong>Sparse evidence exists for any clinical benefit from a POCUS-integrated diagnostic pathway. The results from this trial will help clarify the promising signals for POCUS to influence patient care among ED patients with dyspnea.</p>\",\"PeriodicalId\":45096,\"journal\":{\"name\":\"Open Access Emergency Medicine\",\"volume\":\"16 \",\"pages\":\"211-219\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11365495/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Emergency Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S454062\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S454062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Effect of a Point-of-Care Ultrasound-Driven vs Standard Diagnostic Pathway on 24-Hour Hospital Stay in Emergency Department Patients with Dyspnea-Protocol for A Randomized Controlled Trial.
Purpose: Point-of-care ultrasound (POCUS) helps emergency department (ED) physicians make prompt and appropriate decisions, but the optimal diagnostic integration and potential clinical benefits remain unclear. We describe the protocol and statistical analysis plan for a randomized controlled trial. The objective is to determine the effect of a POCUS-driven diagnostic pathway in adult dyspneic ED patients on the proportion of patients having a hospital stay of less than 24 hours when compared to the standard diagnostic pathway.
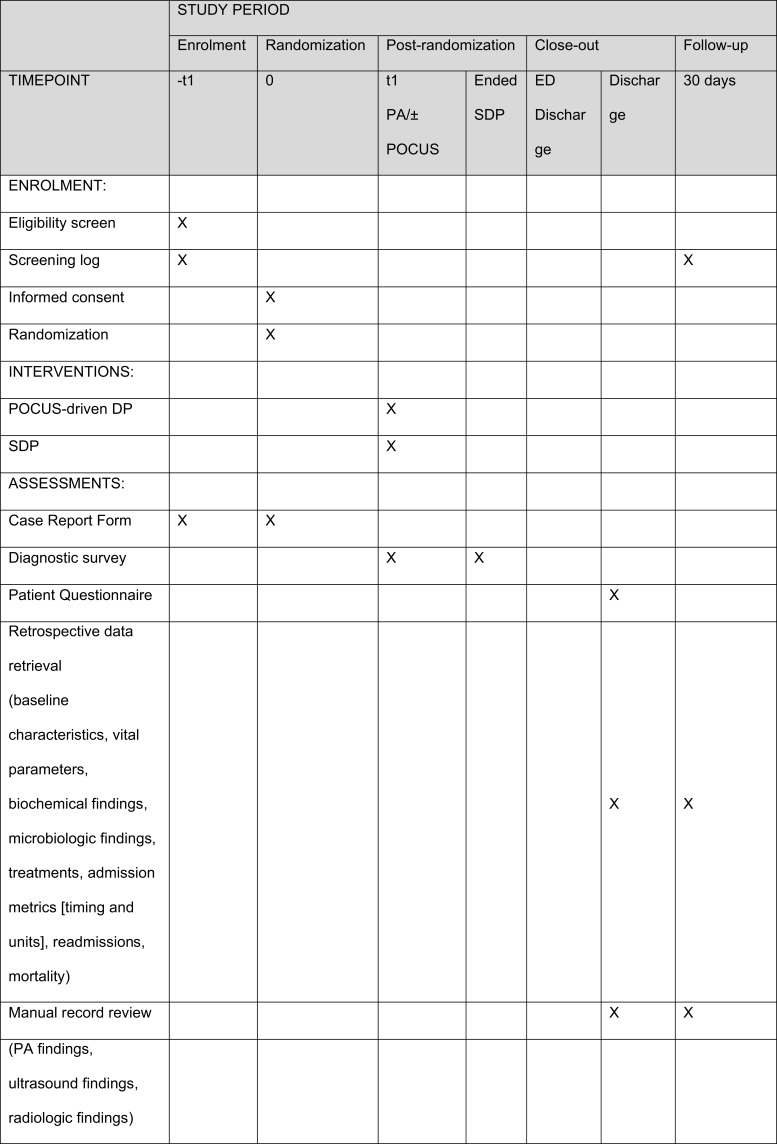
Patients and methods: This is a multicenter, randomized, investigator-initiated, open-labeled, pragmatic, controlled trial. Adult ED patients with chief complaint dyspnea are eligible. Patients are randomized (1:1) to the POCUS-driven diagnostic pathway or standard diagnostic pathway, with 337 patients in each group. The primary outcome is the proportion of patients having a hospital stay (from ED arrival to hospital discharge) of less than 24 hours. Key secondary outcomes include hospital length-of-stay, 72-hour revisits, and 30-day hospital-free days.
Conclusion: Sparse evidence exists for any clinical benefit from a POCUS-integrated diagnostic pathway. The results from this trial will help clarify the promising signals for POCUS to influence patient care among ED patients with dyspnea.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
