Nathan Reynolds, Wei Wei, Kimberly Maroli, Amanda Bonham, Amanda Nizam, Timothy D Gilligan, Christopher Wee, Shilpa Gupta, Moshe C Ornstein
{"title":"不符合一线临床试验条件的转移性肾细胞癌 (mRCC) 患者的临床结果。","authors":"Nathan Reynolds, Wei Wei, Kimberly Maroli, Amanda Bonham, Amanda Nizam, Timothy D Gilligan, Christopher Wee, Shilpa Gupta, Moshe C Ornstein","doi":"10.15586/jkcvhl.v11i3.352","DOIUrl":null,"url":null,"abstract":"<p><p>Clinical trials for immunotherapy-based regimens in metastatic renal cell carcinoma (mRCC) have extensive inclusion and exclusion criteria. We investigated the clinical outcomes in a real-world cohort of patients who would not have met the criteria for inclusion in front-line mRCC trials. Patients treated with ipilimumab/nivolumab and axitinib/pembrolizumab for front-line mRCC were identified and divided into clinical trial eligible (CTE) and clinical trial ineligible (CTI) cohorts based on key inclusion or exclusion criteria from their respective Phase-3 registration trials. Clinical outcomes were compared in CTE and CTI cohorts. A total of 62 patients treated with axitinib/pembrolizumab and 103 treated with ipilimumab/nivolumab were identified. The International Metastatic RCC Database Consortium (IMDC) criteria were similar across CTE and CTI patients in axitinib/pembrolizumab and ipilimumab/nivolumab cohorts. In the axitinib/pembrolizumab cohort (n = 62), 24 (39%) patients were CTI. The major reasons for the ineligibility were lab abnormalities (n = 11), histology (n = 9), and brain metastases (n = 3). There was no significant difference in response rates (P = 0.08). The median progression-free survival (PFS) was numerically longer in CTE patients (28 vs 12 months; P = 0.09). The overall survival (OS) was higher in the CTE patients (P = 0.02). In the ipilimumab/nivolumab cohort (n = 103), 59 (57%) were CTI. The most common reasons for ineligibility were brain metastases (n = 18), lab abnormalities (n = 16), and histology (n = 16). There was no significant difference in response rates (P = 0.22). However, PFS (P = 0.003) and OS (P < 0.0001) were higher in the CTE patients. In conclusion, many real-world patients are ineligible for RCC clinical trials and had worse outcomes when compared to trial-eligible patients. Additional treatment options are needed for these patients, as well as strategies to include them in prospective trials.</p>","PeriodicalId":44291,"journal":{"name":"Journal of Kidney Cancer and VHL","volume":"11 3","pages":"51-58"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11370811/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes for Metastatic Renal Cell Carcinoma (mRCC) Patients Ineligible for Front-line Clinical Trials.\",\"authors\":\"Nathan Reynolds, Wei Wei, Kimberly Maroli, Amanda Bonham, Amanda Nizam, Timothy D Gilligan, Christopher Wee, Shilpa Gupta, Moshe C Ornstein\",\"doi\":\"10.15586/jkcvhl.v11i3.352\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Clinical trials for immunotherapy-based regimens in metastatic renal cell carcinoma (mRCC) have extensive inclusion and exclusion criteria. We investigated the clinical outcomes in a real-world cohort of patients who would not have met the criteria for inclusion in front-line mRCC trials. Patients treated with ipilimumab/nivolumab and axitinib/pembrolizumab for front-line mRCC were identified and divided into clinical trial eligible (CTE) and clinical trial ineligible (CTI) cohorts based on key inclusion or exclusion criteria from their respective Phase-3 registration trials. Clinical outcomes were compared in CTE and CTI cohorts. A total of 62 patients treated with axitinib/pembrolizumab and 103 treated with ipilimumab/nivolumab were identified. The International Metastatic RCC Database Consortium (IMDC) criteria were similar across CTE and CTI patients in axitinib/pembrolizumab and ipilimumab/nivolumab cohorts. In the axitinib/pembrolizumab cohort (n = 62), 24 (39%) patients were CTI. The major reasons for the ineligibility were lab abnormalities (n = 11), histology (n = 9), and brain metastases (n = 3). There was no significant difference in response rates (P = 0.08). The median progression-free survival (PFS) was numerically longer in CTE patients (28 vs 12 months; P = 0.09). The overall survival (OS) was higher in the CTE patients (P = 0.02). In the ipilimumab/nivolumab cohort (n = 103), 59 (57%) were CTI. The most common reasons for ineligibility were brain metastases (n = 18), lab abnormalities (n = 16), and histology (n = 16). There was no significant difference in response rates (P = 0.22). However, PFS (P = 0.003) and OS (P < 0.0001) were higher in the CTE patients. In conclusion, many real-world patients are ineligible for RCC clinical trials and had worse outcomes when compared to trial-eligible patients. Additional treatment options are needed for these patients, as well as strategies to include them in prospective trials.</p>\",\"PeriodicalId\":44291,\"journal\":{\"name\":\"Journal of Kidney Cancer and VHL\",\"volume\":\"11 3\",\"pages\":\"51-58\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11370811/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Kidney Cancer and VHL\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15586/jkcvhl.v11i3.352\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Kidney Cancer and VHL","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15586/jkcvhl.v11i3.352","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Clinical Outcomes for Metastatic Renal Cell Carcinoma (mRCC) Patients Ineligible for Front-line Clinical Trials.
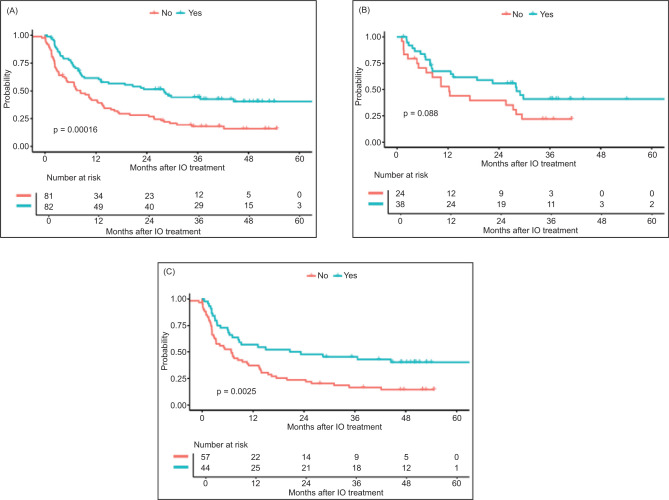
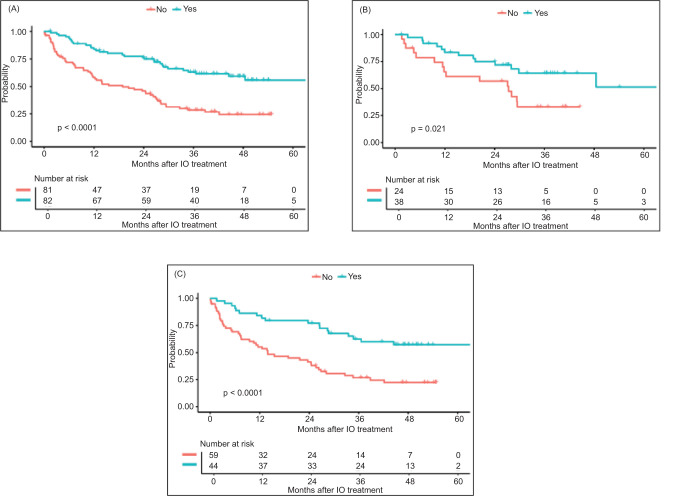
Clinical trials for immunotherapy-based regimens in metastatic renal cell carcinoma (mRCC) have extensive inclusion and exclusion criteria. We investigated the clinical outcomes in a real-world cohort of patients who would not have met the criteria for inclusion in front-line mRCC trials. Patients treated with ipilimumab/nivolumab and axitinib/pembrolizumab for front-line mRCC were identified and divided into clinical trial eligible (CTE) and clinical trial ineligible (CTI) cohorts based on key inclusion or exclusion criteria from their respective Phase-3 registration trials. Clinical outcomes were compared in CTE and CTI cohorts. A total of 62 patients treated with axitinib/pembrolizumab and 103 treated with ipilimumab/nivolumab were identified. The International Metastatic RCC Database Consortium (IMDC) criteria were similar across CTE and CTI patients in axitinib/pembrolizumab and ipilimumab/nivolumab cohorts. In the axitinib/pembrolizumab cohort (n = 62), 24 (39%) patients were CTI. The major reasons for the ineligibility were lab abnormalities (n = 11), histology (n = 9), and brain metastases (n = 3). There was no significant difference in response rates (P = 0.08). The median progression-free survival (PFS) was numerically longer in CTE patients (28 vs 12 months; P = 0.09). The overall survival (OS) was higher in the CTE patients (P = 0.02). In the ipilimumab/nivolumab cohort (n = 103), 59 (57%) were CTI. The most common reasons for ineligibility were brain metastases (n = 18), lab abnormalities (n = 16), and histology (n = 16). There was no significant difference in response rates (P = 0.22). However, PFS (P = 0.003) and OS (P < 0.0001) were higher in the CTE patients. In conclusion, many real-world patients are ineligible for RCC clinical trials and had worse outcomes when compared to trial-eligible patients. Additional treatment options are needed for these patients, as well as strategies to include them in prospective trials.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
