Kai Hübel, Mark Bower, Igor Aurer, Mariana Bastos-Oreiro, Caroline Besson, Uta Brunnberg, Chiara Cattaneo, Simon Collins, Kate Cwynarski, Alessia D. Pria, Marcus Hentrich, Christian Hoffmann, Marie J. Kersten, Silvia Montoto, Jose-Tomas Navarro, Eric Oksenhendler, Alessandro Re, Josep-Maria Ribera, Philipp Schommers, Bastian von Tresckow, Christian Buske, Martin Dreyling, Andy Davies, the EHA and ESMO Guidelines Committees
{"title":"人体免疫缺陷病毒相关淋巴瘤:EHA-ESMO 诊断、治疗和随访临床实践指南","authors":"Kai Hübel, Mark Bower, Igor Aurer, Mariana Bastos-Oreiro, Caroline Besson, Uta Brunnberg, Chiara Cattaneo, Simon Collins, Kate Cwynarski, Alessia D. Pria, Marcus Hentrich, Christian Hoffmann, Marie J. Kersten, Silvia Montoto, Jose-Tomas Navarro, Eric Oksenhendler, Alessandro Re, Josep-Maria Ribera, Philipp Schommers, Bastian von Tresckow, Christian Buske, Martin Dreyling, Andy Davies, the EHA and ESMO Guidelines Committees","doi":"10.1002/hem3.150","DOIUrl":null,"url":null,"abstract":"<p>Non-Hodgkin lymphoma (NHL) remains the most common type of cancer and a leading cause of mortality in people who are living with human immunodeficiency virus (HIV).<span><sup>1</sup></span> This is despite a marked decrease in the incidence of HIV-associated NHL (HIV–NHL) following the introduction of combination antiretroviral therapy (ART) in the mid-1990s.<span><sup>2</sup></span> In contrast, the incidence of Hodgkin lymphoma (HL) increased slightly but has remained stable since 2000.<span><sup>1</sup></span> Compared with the age- and gender-matched general population, the incidences of HIV–NHL and HIV-associated HL (HIV–HL) are increased ~10- to 20-fold.<span><sup>3</sup></span></p><p>The most common histological types of HIV-associated lymphomas are diffuse large B-cell lymphoma (DLBCL; 37%), HL (26%) and Burkitt lymphoma (BL; 20%).<span><sup>4</sup></span> Independent risk factors for DLBCL in people living with HIV (PLWH) include a low cluster of differentiation (CD)4 T-cell count and an uncontrolled HIV-1 viral load (VL).<span><sup>5</sup></span> The availability of ART and better management of opportunistic infections allow PLWH to receive the same treatments as people without HIV, including intensive therapies, such as autologous stem-cell transplantation (ASCT), allogeneic stem-cell transplantation (allo-SCT) and chimeric antigen receptor T-cell (CAR-T) therapy. Patients with HIV-associated lymphomas should be enrolled in clinical trials whenever possible.</p><p>The aim of this guideline is to provide practical clinical guidance and recommendations to clinicians who manage HIV-associated lymphomas.</p><p>Diagnostic procedures in patients with HIV-associated lymphoma generally mirror those recommended for lymphoma in the general population and those necessary to assess the severity and complications of HIV and its treatment (see Supporting Information S1: Table S1).</p><p>Lymphoma should be diagnosed via tumour biopsy, preferably excisional, that is evaluated by an expert haematopathologist using immunohistochemistry (IHC) and molecular techniques. In exceptional cases when no tumour mass can be biopsied, diagnosis can be made by cytology and flow cytometry.</p><p>Lymphoma staging should involve a contrast-enhanced computed tomography (CT) scan of the neck, chest, abdomen and pelvis and a bone marrow biopsy. A staging [<sup>18</sup>F]2-fluoro-2-deoxy-<span>d</span>-glucose (FDG)–positron emission tomography (PET)–CT scan is more sensitive, especially for extranodal disease. FDG–PET–CT may, however, have a higher false-positive rate in PLWH due to immune deficiency-related lymphoid hyperplasia and non-suppressed HIV infection.<span><sup>6</sup></span> Interim FDG–PET–CT (iFDG–PET–CT) results should, therefore, be interpreted cautiously if used to escalate treatment and when analysing end-of-treatment response; if there is doubt, FDG-avid lesions should be re-biopsied. Otherwise, response criteria do not differ from those used in immunocompetent individuals.</p><p>Magnetic resonance imaging (MRI) is the optimal method for staging and response assessment of central nervous system (CNS) lymphomas. Cerebral opportunistic infections may, however, mimic lymphoma in PLWH. Small case series suggest that FDG–PET–CT can differentiate between cerebral infections, such as toxoplasmosis,<span><sup>7</sup></span> and CNS lymphoma, but biopsy (preferably stereotactic) remains the gold standard for diagnosis.</p><p>All additional investigations for patients with newly diagnosed HIV should follow the annually updated, evidence-graded European Acquired Immune Deficiency Syndrome Clinical Society guidelines, available at http://www.eacsociety.org/guidelines/eacs-guidelines/.</p><p>The main risk factor for HL in the HIV setting is a moderately lowered CD4 count.<span><sup>5</sup></span> In a recent study, the hazard ratio for HL was highest (6.36) among patients with CD4 counts of 100–200 cells/µL compared with the reference group (CD4 counts >500 cells/µL).<span><sup>5</sup></span> In contrast, higher HIV-1 VL (>50 copies/mL) was not associated with an increased risk of HL compared with a VL of ≤50 copies/mL.<span><sup>5</sup></span></p><p>HHV-8-associated MCD (HHV-8–MCD) is a rare lymphoproliferative disorder that is predominantly associated with HIV infection. Incidence does not correlate with CD4 count or HIV plasma viraemia.</p><p>This Clinical Practice Guideline (CPG) was developed in accordance with the ESMO standard operating procedures for CPG development (https://www.esmo.org/Guidelines/ESMO-Guidelines-Methodology). The relevant literature has been selected by the expert authors. The FDA/EMA or other regulatory body approval status of new therapies/indications is reported at the time of writing this CPG. Levels of evidence and grades of recommendation have been applied using the system shown in Supporting Information S1: Table S4. Statements without grading were considered justified standard clinical practice by the authors. The guideline uses people-first terminology. For future updates to this CPG, including eUpdates and Living Guidelines, please see the ESMO Guidelines website: https://www.esmo.org/guidelines/guidelines-by-topic/haematological-malignancies.</p><p>All authors conceptualised, wrote and approved the final version.</p><p>KH reports personal fees for advisory board membership from Gilead, Hexal, Incyte, Miltenyi, Novartis, Recordati and Roche; personal fees as an invited speaker from BeiGene, Bristol Myers Squibb (BMS), Novartis, Recordati, Roche and Servier; personal fees for a writing engagement from Hexal; institutional fees as coordinating Principal Investigator (PI) from Incyte and Roche; a non-renumerated role as working group chair of the German Society of Hematology and Medical Oncology (DGHO); non-remunerated advisory role for the European Hematology Association (EHA) Education Committee; and a non-remunerated leadership role for the German Lymphoma Alliance. MB reports personal fees as an invited speaker from BMS, EUSA Pharma, Gilead, Janssen, Merck and ViiV Healthcare. IA reports personal fees for advisory board membership from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sandoz, Sobi and Takeda; non-remunerated leadership roles for the Croatian Cooperative Group for Hematologic Diseases and the EHA Lymphoma Specialized Working Group; and non-renumerated membership of the Board of Directors of the Croatian Hematological Society and the European Lymphoma Institute. MBO reports personal fees for advisory board participation from Kite Pharma, Novartis and Roche; personal fees as an invited speaker from Janssen, Kite Pharma, Roche and Takeda; a personal and institutional research grant from Kite Pharma (Gilead/Kite Pharma award); and non-renumerated leadership roles for the Spanish Lymphoma Group (GELTAMO; coordinator of the Aggressive Group and member of the Scientific Committee), the Madrid Hematology Society (member of the Board of Directors, treasurer) and the Spanish Society of Hematology and Hemotherapy (member of the Board of Directors, accountant). CBe reports personal fees for expert testimony from Janssen. UB reports personal fees for advisory board membership from Janssen-Cilag; personal fees as an invited speaker from AstraZeneca and Janssen-Cilag; personal fees for writing engagements from AbbVie and AstraZeneca; travel grants from AbbVie, BeiGene and Gilead; compensation for congress registration fees from Lilly; a non-renumerated role as PI for Regeneron and Roche; and non-renumerated membership of DGHO, the German Cancer Society (DKG) and EHA. CC reports no conflicts of interest. SC reports employment as a treatment advocate by the charity HIV i-Base. KC reports personal fees for advisory board membership from AbbVie, Atara, Celgene, Incyte, Janssen, Kite, Roche and Takeda; personal fees as an invited speaker and personal travel grants/conference support from Celgene, Incyte, Kite, Roche and Takeda; personal fees for consulting from Atara, Celgene, Incyte and Kite. ADP reports institutional fees as an invited speaker from Gilead (non-promotional teaching). MH reports personal fees for advisory board membership from Amgen, EUSA Pharma, Sanofi, Stemline and Takeda; and personal fees as an invited speaker from EUSA Pharma, Gilead, Janssen, Jazz Pharmaceuticals and Sanofi. CH reports personal fees for advisory board membership and as an invited speaker from EUSA Pharma, Gilead Sciences, Janssen-Cilag, MSD and ViiV Healthcare; and institutional fees as local PI (for clinical studies conducted at institution) from Janssen-Cilag, MSD and ViiV Healthcare. MJK reports institutional fees for advisory board membership from Adicet Bio, BMS/Celgene, Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis; institutional fees as an invited speaker from BeiGene, BMS/Celgene, Kite (a Gilead Company) and Novartis; institutional fees as local PI from BMS/Celgene; institutional fees as coordinating PI from Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis, and an institutional travel grant from AbbVie. SM reports personal fees for participation in a Data Monitoring Committee from Bayer. JTN reports personal fees for advisory board membership from Recordati Rare Diseases EUSA Pharma; personal fees as an invited speaker from Novartis and Recordati Rare Diseases EUSA Pharma; a personal research grant from Gilead Spain; and institutional funding from Recordati Rare Diseases EUSA Pharma. EO reports personal fees as an expert for grant attributions from CSL Behring; personal fees as a consultant from EUSA Pharma; an institutional research grant on unicentric Castleman disease pathogenesis from the Castleman Disease Collaborative Network (CDCN); and non-renumerated membership of the advisory board of CDCN. AR reports personal fees for advisory board membership from Incyte, Italfarmaco and Takeda; personal fees as an expert discussant from Janssen and Servier; personal fees as an invited speaker from Sobi and Takeda; institutional fees as local PI from MSD, Pharmacyclis and Sanofi. JMR reports personal fees for advisory board membership from Amgen, Pfizer, Shire and Takeda; personal fees as an invited speaker from Amgen; and personal fees as local PI from Takeda. PS reports personal fees as an invited speaker from MSD and ViiV Healthcare; and a personal and institutional research grant from Gilead Sciences. BvT reports personal fees for advisory and consultancy roles for Allogene, Amgen, BMS/Celgene, Cerus, Gilead Kite, Incyte, IQVIA, Janssen-Cilag GmbH, Lilly, Miltenyi, MSD, Noscendo, Novartis, Pentixapharm, Pfizer, Pierre Fabre, QualWorld, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, BMS/Celgene, Gilead Kite, Incyte, Lilly, MSD, Novartis, Roche Pharma AG and Takeda; institutional funding from Esteve, MSD, Novartis and Takeda; and travel support from AbbVie, AstraZeneca, Gilead Kite, Lilly, MSD, Pierre Fabre, Roche, Takeda and Novartis. CBu reports personal fees for advisory board membership from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; personal fees as an invited speaker from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; and institutional funding from AbbVie Amgen, Bayer, Celltrion, Janssen, MSD, Pfizer and Roche (all for investigator-sponsored clinical trials and registries). MD reports personal fees as an advisory board member from AbbVie, AstraZeneca, BeiGene, BMS/Celgene, Gilead, Janssen, Lilly/Loxo, Novartis and Roche; personal fees as an invited speaker for AstraZeneca, BeiGene, Gilead/Kite, Janssen, Lilly, Novartis and Roche; institutional research grants from AbbVie, Bayer, Celgene, Janssen, Lilly and Roche; institutional funding from Gilead/Kite; and non-renumerated membership of the American Society of Clinical Oncology, American Society of Hematology (subcommittee), DGHO (prior Board member), EHA (Executive Board), ESMO (Faculty) and the Lymphoma Research Foundation (Mantle Cell Lymphoma Consortium). AD reports personal fees as an advisory board member for AbbVie, Acerta Pharma, AstraZeneca, BMS/Celgene, Genmab, Gilead, Incyte, Karyopharm, Kite Pharma, Regeneron, Roche, Sobi and Takeda; personal fees as an invited speaker for AstraZeneca, Gilead and Roche; institutional research grants for conduct of commercial research and funding of IST from Acerta Pharma and Roche; institutional research grants for conduct of commercial research from ADC Therapeutics, AstraZeneca, BMS/Celgene, Gilead and Pfizer; institutional research grant from MSD (no financial interest); non-renumerated leadership role, member and UK Board representative for the Precision Medicine in Aggressive Lymphoma Consortium of the International Extranodal Lymphoma Study Group; advisory role and international advisor for the Swiss SAKK Lymphoma Project Group and member of the UK National Cancer Research Institute's High Grade Lymphoma Study Group.</p><p>No external funding has been received for the preparation of this guideline. Production costs have been covered by ESMO (for <i>Annals of Oncology</i>) and EHA (for <i>HemaSphere</i>) central funds.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 9","pages":""},"PeriodicalIF":11.3000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.150","citationCount":"0","resultStr":"{\"title\":\"Human immunodeficiency virus-associated Lymphomas: EHA–ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up\",\"authors\":\"Kai Hübel, Mark Bower, Igor Aurer, Mariana Bastos-Oreiro, Caroline Besson, Uta Brunnberg, Chiara Cattaneo, Simon Collins, Kate Cwynarski, Alessia D. Pria, Marcus Hentrich, Christian Hoffmann, Marie J. Kersten, Silvia Montoto, Jose-Tomas Navarro, Eric Oksenhendler, Alessandro Re, Josep-Maria Ribera, Philipp Schommers, Bastian von Tresckow, Christian Buske, Martin Dreyling, Andy Davies, the EHA and ESMO Guidelines Committees\",\"doi\":\"10.1002/hem3.150\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Non-Hodgkin lymphoma (NHL) remains the most common type of cancer and a leading cause of mortality in people who are living with human immunodeficiency virus (HIV).<span><sup>1</sup></span> This is despite a marked decrease in the incidence of HIV-associated NHL (HIV–NHL) following the introduction of combination antiretroviral therapy (ART) in the mid-1990s.<span><sup>2</sup></span> In contrast, the incidence of Hodgkin lymphoma (HL) increased slightly but has remained stable since 2000.<span><sup>1</sup></span> Compared with the age- and gender-matched general population, the incidences of HIV–NHL and HIV-associated HL (HIV–HL) are increased ~10- to 20-fold.<span><sup>3</sup></span></p><p>The most common histological types of HIV-associated lymphomas are diffuse large B-cell lymphoma (DLBCL; 37%), HL (26%) and Burkitt lymphoma (BL; 20%).<span><sup>4</sup></span> Independent risk factors for DLBCL in people living with HIV (PLWH) include a low cluster of differentiation (CD)4 T-cell count and an uncontrolled HIV-1 viral load (VL).<span><sup>5</sup></span> The availability of ART and better management of opportunistic infections allow PLWH to receive the same treatments as people without HIV, including intensive therapies, such as autologous stem-cell transplantation (ASCT), allogeneic stem-cell transplantation (allo-SCT) and chimeric antigen receptor T-cell (CAR-T) therapy. Patients with HIV-associated lymphomas should be enrolled in clinical trials whenever possible.</p><p>The aim of this guideline is to provide practical clinical guidance and recommendations to clinicians who manage HIV-associated lymphomas.</p><p>Diagnostic procedures in patients with HIV-associated lymphoma generally mirror those recommended for lymphoma in the general population and those necessary to assess the severity and complications of HIV and its treatment (see Supporting Information S1: Table S1).</p><p>Lymphoma should be diagnosed via tumour biopsy, preferably excisional, that is evaluated by an expert haematopathologist using immunohistochemistry (IHC) and molecular techniques. In exceptional cases when no tumour mass can be biopsied, diagnosis can be made by cytology and flow cytometry.</p><p>Lymphoma staging should involve a contrast-enhanced computed tomography (CT) scan of the neck, chest, abdomen and pelvis and a bone marrow biopsy. A staging [<sup>18</sup>F]2-fluoro-2-deoxy-<span>d</span>-glucose (FDG)–positron emission tomography (PET)–CT scan is more sensitive, especially for extranodal disease. FDG–PET–CT may, however, have a higher false-positive rate in PLWH due to immune deficiency-related lymphoid hyperplasia and non-suppressed HIV infection.<span><sup>6</sup></span> Interim FDG–PET–CT (iFDG–PET–CT) results should, therefore, be interpreted cautiously if used to escalate treatment and when analysing end-of-treatment response; if there is doubt, FDG-avid lesions should be re-biopsied. Otherwise, response criteria do not differ from those used in immunocompetent individuals.</p><p>Magnetic resonance imaging (MRI) is the optimal method for staging and response assessment of central nervous system (CNS) lymphomas. Cerebral opportunistic infections may, however, mimic lymphoma in PLWH. Small case series suggest that FDG–PET–CT can differentiate between cerebral infections, such as toxoplasmosis,<span><sup>7</sup></span> and CNS lymphoma, but biopsy (preferably stereotactic) remains the gold standard for diagnosis.</p><p>All additional investigations for patients with newly diagnosed HIV should follow the annually updated, evidence-graded European Acquired Immune Deficiency Syndrome Clinical Society guidelines, available at http://www.eacsociety.org/guidelines/eacs-guidelines/.</p><p>The main risk factor for HL in the HIV setting is a moderately lowered CD4 count.<span><sup>5</sup></span> In a recent study, the hazard ratio for HL was highest (6.36) among patients with CD4 counts of 100–200 cells/µL compared with the reference group (CD4 counts >500 cells/µL).<span><sup>5</sup></span> In contrast, higher HIV-1 VL (>50 copies/mL) was not associated with an increased risk of HL compared with a VL of ≤50 copies/mL.<span><sup>5</sup></span></p><p>HHV-8-associated MCD (HHV-8–MCD) is a rare lymphoproliferative disorder that is predominantly associated with HIV infection. Incidence does not correlate with CD4 count or HIV plasma viraemia.</p><p>This Clinical Practice Guideline (CPG) was developed in accordance with the ESMO standard operating procedures for CPG development (https://www.esmo.org/Guidelines/ESMO-Guidelines-Methodology). The relevant literature has been selected by the expert authors. The FDA/EMA or other regulatory body approval status of new therapies/indications is reported at the time of writing this CPG. Levels of evidence and grades of recommendation have been applied using the system shown in Supporting Information S1: Table S4. Statements without grading were considered justified standard clinical practice by the authors. The guideline uses people-first terminology. For future updates to this CPG, including eUpdates and Living Guidelines, please see the ESMO Guidelines website: https://www.esmo.org/guidelines/guidelines-by-topic/haematological-malignancies.</p><p>All authors conceptualised, wrote and approved the final version.</p><p>KH reports personal fees for advisory board membership from Gilead, Hexal, Incyte, Miltenyi, Novartis, Recordati and Roche; personal fees as an invited speaker from BeiGene, Bristol Myers Squibb (BMS), Novartis, Recordati, Roche and Servier; personal fees for a writing engagement from Hexal; institutional fees as coordinating Principal Investigator (PI) from Incyte and Roche; a non-renumerated role as working group chair of the German Society of Hematology and Medical Oncology (DGHO); non-remunerated advisory role for the European Hematology Association (EHA) Education Committee; and a non-remunerated leadership role for the German Lymphoma Alliance. MB reports personal fees as an invited speaker from BMS, EUSA Pharma, Gilead, Janssen, Merck and ViiV Healthcare. IA reports personal fees for advisory board membership from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sandoz, Sobi and Takeda; non-remunerated leadership roles for the Croatian Cooperative Group for Hematologic Diseases and the EHA Lymphoma Specialized Working Group; and non-renumerated membership of the Board of Directors of the Croatian Hematological Society and the European Lymphoma Institute. MBO reports personal fees for advisory board participation from Kite Pharma, Novartis and Roche; personal fees as an invited speaker from Janssen, Kite Pharma, Roche and Takeda; a personal and institutional research grant from Kite Pharma (Gilead/Kite Pharma award); and non-renumerated leadership roles for the Spanish Lymphoma Group (GELTAMO; coordinator of the Aggressive Group and member of the Scientific Committee), the Madrid Hematology Society (member of the Board of Directors, treasurer) and the Spanish Society of Hematology and Hemotherapy (member of the Board of Directors, accountant). CBe reports personal fees for expert testimony from Janssen. UB reports personal fees for advisory board membership from Janssen-Cilag; personal fees as an invited speaker from AstraZeneca and Janssen-Cilag; personal fees for writing engagements from AbbVie and AstraZeneca; travel grants from AbbVie, BeiGene and Gilead; compensation for congress registration fees from Lilly; a non-renumerated role as PI for Regeneron and Roche; and non-renumerated membership of DGHO, the German Cancer Society (DKG) and EHA. CC reports no conflicts of interest. SC reports employment as a treatment advocate by the charity HIV i-Base. KC reports personal fees for advisory board membership from AbbVie, Atara, Celgene, Incyte, Janssen, Kite, Roche and Takeda; personal fees as an invited speaker and personal travel grants/conference support from Celgene, Incyte, Kite, Roche and Takeda; personal fees for consulting from Atara, Celgene, Incyte and Kite. ADP reports institutional fees as an invited speaker from Gilead (non-promotional teaching). MH reports personal fees for advisory board membership from Amgen, EUSA Pharma, Sanofi, Stemline and Takeda; and personal fees as an invited speaker from EUSA Pharma, Gilead, Janssen, Jazz Pharmaceuticals and Sanofi. CH reports personal fees for advisory board membership and as an invited speaker from EUSA Pharma, Gilead Sciences, Janssen-Cilag, MSD and ViiV Healthcare; and institutional fees as local PI (for clinical studies conducted at institution) from Janssen-Cilag, MSD and ViiV Healthcare. MJK reports institutional fees for advisory board membership from Adicet Bio, BMS/Celgene, Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis; institutional fees as an invited speaker from BeiGene, BMS/Celgene, Kite (a Gilead Company) and Novartis; institutional fees as local PI from BMS/Celgene; institutional fees as coordinating PI from Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis, and an institutional travel grant from AbbVie. SM reports personal fees for participation in a Data Monitoring Committee from Bayer. JTN reports personal fees for advisory board membership from Recordati Rare Diseases EUSA Pharma; personal fees as an invited speaker from Novartis and Recordati Rare Diseases EUSA Pharma; a personal research grant from Gilead Spain; and institutional funding from Recordati Rare Diseases EUSA Pharma. EO reports personal fees as an expert for grant attributions from CSL Behring; personal fees as a consultant from EUSA Pharma; an institutional research grant on unicentric Castleman disease pathogenesis from the Castleman Disease Collaborative Network (CDCN); and non-renumerated membership of the advisory board of CDCN. AR reports personal fees for advisory board membership from Incyte, Italfarmaco and Takeda; personal fees as an expert discussant from Janssen and Servier; personal fees as an invited speaker from Sobi and Takeda; institutional fees as local PI from MSD, Pharmacyclis and Sanofi. JMR reports personal fees for advisory board membership from Amgen, Pfizer, Shire and Takeda; personal fees as an invited speaker from Amgen; and personal fees as local PI from Takeda. PS reports personal fees as an invited speaker from MSD and ViiV Healthcare; and a personal and institutional research grant from Gilead Sciences. BvT reports personal fees for advisory and consultancy roles for Allogene, Amgen, BMS/Celgene, Cerus, Gilead Kite, Incyte, IQVIA, Janssen-Cilag GmbH, Lilly, Miltenyi, MSD, Noscendo, Novartis, Pentixapharm, Pfizer, Pierre Fabre, QualWorld, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, BMS/Celgene, Gilead Kite, Incyte, Lilly, MSD, Novartis, Roche Pharma AG and Takeda; institutional funding from Esteve, MSD, Novartis and Takeda; and travel support from AbbVie, AstraZeneca, Gilead Kite, Lilly, MSD, Pierre Fabre, Roche, Takeda and Novartis. CBu reports personal fees for advisory board membership from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; personal fees as an invited speaker from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; and institutional funding from AbbVie Amgen, Bayer, Celltrion, Janssen, MSD, Pfizer and Roche (all for investigator-sponsored clinical trials and registries). MD reports personal fees as an advisory board member from AbbVie, AstraZeneca, BeiGene, BMS/Celgene, Gilead, Janssen, Lilly/Loxo, Novartis and Roche; personal fees as an invited speaker for AstraZeneca, BeiGene, Gilead/Kite, Janssen, Lilly, Novartis and Roche; institutional research grants from AbbVie, Bayer, Celgene, Janssen, Lilly and Roche; institutional funding from Gilead/Kite; and non-renumerated membership of the American Society of Clinical Oncology, American Society of Hematology (subcommittee), DGHO (prior Board member), EHA (Executive Board), ESMO (Faculty) and the Lymphoma Research Foundation (Mantle Cell Lymphoma Consortium). AD reports personal fees as an advisory board member for AbbVie, Acerta Pharma, AstraZeneca, BMS/Celgene, Genmab, Gilead, Incyte, Karyopharm, Kite Pharma, Regeneron, Roche, Sobi and Takeda; personal fees as an invited speaker for AstraZeneca, Gilead and Roche; institutional research grants for conduct of commercial research and funding of IST from Acerta Pharma and Roche; institutional research grants for conduct of commercial research from ADC Therapeutics, AstraZeneca, BMS/Celgene, Gilead and Pfizer; institutional research grant from MSD (no financial interest); non-renumerated leadership role, member and UK Board representative for the Precision Medicine in Aggressive Lymphoma Consortium of the International Extranodal Lymphoma Study Group; advisory role and international advisor for the Swiss SAKK Lymphoma Project Group and member of the UK National Cancer Research Institute's High Grade Lymphoma Study Group.</p><p>No external funding has been received for the preparation of this guideline. Production costs have been covered by ESMO (for <i>Annals of Oncology</i>) and EHA (for <i>HemaSphere</i>) central funds.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 9\",\"pages\":\"\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.150\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.150\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.150","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Human immunodeficiency virus-associated Lymphomas: EHA–ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up
Non-Hodgkin lymphoma (NHL) remains the most common type of cancer and a leading cause of mortality in people who are living with human immunodeficiency virus (HIV).1 This is despite a marked decrease in the incidence of HIV-associated NHL (HIV–NHL) following the introduction of combination antiretroviral therapy (ART) in the mid-1990s.2 In contrast, the incidence of Hodgkin lymphoma (HL) increased slightly but has remained stable since 2000.1 Compared with the age- and gender-matched general population, the incidences of HIV–NHL and HIV-associated HL (HIV–HL) are increased ~10- to 20-fold.3
The most common histological types of HIV-associated lymphomas are diffuse large B-cell lymphoma (DLBCL; 37%), HL (26%) and Burkitt lymphoma (BL; 20%).4 Independent risk factors for DLBCL in people living with HIV (PLWH) include a low cluster of differentiation (CD)4 T-cell count and an uncontrolled HIV-1 viral load (VL).5 The availability of ART and better management of opportunistic infections allow PLWH to receive the same treatments as people without HIV, including intensive therapies, such as autologous stem-cell transplantation (ASCT), allogeneic stem-cell transplantation (allo-SCT) and chimeric antigen receptor T-cell (CAR-T) therapy. Patients with HIV-associated lymphomas should be enrolled in clinical trials whenever possible.
The aim of this guideline is to provide practical clinical guidance and recommendations to clinicians who manage HIV-associated lymphomas.
Diagnostic procedures in patients with HIV-associated lymphoma generally mirror those recommended for lymphoma in the general population and those necessary to assess the severity and complications of HIV and its treatment (see Supporting Information S1: Table S1).
Lymphoma should be diagnosed via tumour biopsy, preferably excisional, that is evaluated by an expert haematopathologist using immunohistochemistry (IHC) and molecular techniques. In exceptional cases when no tumour mass can be biopsied, diagnosis can be made by cytology and flow cytometry.
Lymphoma staging should involve a contrast-enhanced computed tomography (CT) scan of the neck, chest, abdomen and pelvis and a bone marrow biopsy. A staging [18F]2-fluoro-2-deoxy-d-glucose (FDG)–positron emission tomography (PET)–CT scan is more sensitive, especially for extranodal disease. FDG–PET–CT may, however, have a higher false-positive rate in PLWH due to immune deficiency-related lymphoid hyperplasia and non-suppressed HIV infection.6 Interim FDG–PET–CT (iFDG–PET–CT) results should, therefore, be interpreted cautiously if used to escalate treatment and when analysing end-of-treatment response; if there is doubt, FDG-avid lesions should be re-biopsied. Otherwise, response criteria do not differ from those used in immunocompetent individuals.
Magnetic resonance imaging (MRI) is the optimal method for staging and response assessment of central nervous system (CNS) lymphomas. Cerebral opportunistic infections may, however, mimic lymphoma in PLWH. Small case series suggest that FDG–PET–CT can differentiate between cerebral infections, such as toxoplasmosis,7 and CNS lymphoma, but biopsy (preferably stereotactic) remains the gold standard for diagnosis.
All additional investigations for patients with newly diagnosed HIV should follow the annually updated, evidence-graded European Acquired Immune Deficiency Syndrome Clinical Society guidelines, available at http://www.eacsociety.org/guidelines/eacs-guidelines/.
The main risk factor for HL in the HIV setting is a moderately lowered CD4 count.5 In a recent study, the hazard ratio for HL was highest (6.36) among patients with CD4 counts of 100–200 cells/µL compared with the reference group (CD4 counts >500 cells/µL).5 In contrast, higher HIV-1 VL (>50 copies/mL) was not associated with an increased risk of HL compared with a VL of ≤50 copies/mL.5
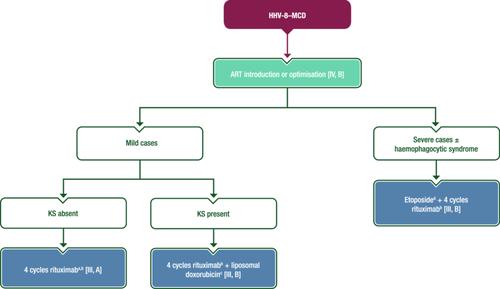
HHV-8-associated MCD (HHV-8–MCD) is a rare lymphoproliferative disorder that is predominantly associated with HIV infection. Incidence does not correlate with CD4 count or HIV plasma viraemia.
This Clinical Practice Guideline (CPG) was developed in accordance with the ESMO standard operating procedures for CPG development (https://www.esmo.org/Guidelines/ESMO-Guidelines-Methodology). The relevant literature has been selected by the expert authors. The FDA/EMA or other regulatory body approval status of new therapies/indications is reported at the time of writing this CPG. Levels of evidence and grades of recommendation have been applied using the system shown in Supporting Information S1: Table S4. Statements without grading were considered justified standard clinical practice by the authors. The guideline uses people-first terminology. For future updates to this CPG, including eUpdates and Living Guidelines, please see the ESMO Guidelines website: https://www.esmo.org/guidelines/guidelines-by-topic/haematological-malignancies.
All authors conceptualised, wrote and approved the final version.
KH reports personal fees for advisory board membership from Gilead, Hexal, Incyte, Miltenyi, Novartis, Recordati and Roche; personal fees as an invited speaker from BeiGene, Bristol Myers Squibb (BMS), Novartis, Recordati, Roche and Servier; personal fees for a writing engagement from Hexal; institutional fees as coordinating Principal Investigator (PI) from Incyte and Roche; a non-renumerated role as working group chair of the German Society of Hematology and Medical Oncology (DGHO); non-remunerated advisory role for the European Hematology Association (EHA) Education Committee; and a non-remunerated leadership role for the German Lymphoma Alliance. MB reports personal fees as an invited speaker from BMS, EUSA Pharma, Gilead, Janssen, Merck and ViiV Healthcare. IA reports personal fees for advisory board membership from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, Eli Lilly, Genesis/Incyte, Janssen, Novartis, Roche, Sandoz, Sobi and Takeda; non-remunerated leadership roles for the Croatian Cooperative Group for Hematologic Diseases and the EHA Lymphoma Specialized Working Group; and non-renumerated membership of the Board of Directors of the Croatian Hematological Society and the European Lymphoma Institute. MBO reports personal fees for advisory board participation from Kite Pharma, Novartis and Roche; personal fees as an invited speaker from Janssen, Kite Pharma, Roche and Takeda; a personal and institutional research grant from Kite Pharma (Gilead/Kite Pharma award); and non-renumerated leadership roles for the Spanish Lymphoma Group (GELTAMO; coordinator of the Aggressive Group and member of the Scientific Committee), the Madrid Hematology Society (member of the Board of Directors, treasurer) and the Spanish Society of Hematology and Hemotherapy (member of the Board of Directors, accountant). CBe reports personal fees for expert testimony from Janssen. UB reports personal fees for advisory board membership from Janssen-Cilag; personal fees as an invited speaker from AstraZeneca and Janssen-Cilag; personal fees for writing engagements from AbbVie and AstraZeneca; travel grants from AbbVie, BeiGene and Gilead; compensation for congress registration fees from Lilly; a non-renumerated role as PI for Regeneron and Roche; and non-renumerated membership of DGHO, the German Cancer Society (DKG) and EHA. CC reports no conflicts of interest. SC reports employment as a treatment advocate by the charity HIV i-Base. KC reports personal fees for advisory board membership from AbbVie, Atara, Celgene, Incyte, Janssen, Kite, Roche and Takeda; personal fees as an invited speaker and personal travel grants/conference support from Celgene, Incyte, Kite, Roche and Takeda; personal fees for consulting from Atara, Celgene, Incyte and Kite. ADP reports institutional fees as an invited speaker from Gilead (non-promotional teaching). MH reports personal fees for advisory board membership from Amgen, EUSA Pharma, Sanofi, Stemline and Takeda; and personal fees as an invited speaker from EUSA Pharma, Gilead, Janssen, Jazz Pharmaceuticals and Sanofi. CH reports personal fees for advisory board membership and as an invited speaker from EUSA Pharma, Gilead Sciences, Janssen-Cilag, MSD and ViiV Healthcare; and institutional fees as local PI (for clinical studies conducted at institution) from Janssen-Cilag, MSD and ViiV Healthcare. MJK reports institutional fees for advisory board membership from Adicet Bio, BMS/Celgene, Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis; institutional fees as an invited speaker from BeiGene, BMS/Celgene, Kite (a Gilead Company) and Novartis; institutional fees as local PI from BMS/Celgene; institutional fees as coordinating PI from Galapagos, Kite (a Gilead Company), Miltenyi Biotec and Novartis, and an institutional travel grant from AbbVie. SM reports personal fees for participation in a Data Monitoring Committee from Bayer. JTN reports personal fees for advisory board membership from Recordati Rare Diseases EUSA Pharma; personal fees as an invited speaker from Novartis and Recordati Rare Diseases EUSA Pharma; a personal research grant from Gilead Spain; and institutional funding from Recordati Rare Diseases EUSA Pharma. EO reports personal fees as an expert for grant attributions from CSL Behring; personal fees as a consultant from EUSA Pharma; an institutional research grant on unicentric Castleman disease pathogenesis from the Castleman Disease Collaborative Network (CDCN); and non-renumerated membership of the advisory board of CDCN. AR reports personal fees for advisory board membership from Incyte, Italfarmaco and Takeda; personal fees as an expert discussant from Janssen and Servier; personal fees as an invited speaker from Sobi and Takeda; institutional fees as local PI from MSD, Pharmacyclis and Sanofi. JMR reports personal fees for advisory board membership from Amgen, Pfizer, Shire and Takeda; personal fees as an invited speaker from Amgen; and personal fees as local PI from Takeda. PS reports personal fees as an invited speaker from MSD and ViiV Healthcare; and a personal and institutional research grant from Gilead Sciences. BvT reports personal fees for advisory and consultancy roles for Allogene, Amgen, BMS/Celgene, Cerus, Gilead Kite, Incyte, IQVIA, Janssen-Cilag GmbH, Lilly, Miltenyi, MSD, Noscendo, Novartis, Pentixapharm, Pfizer, Pierre Fabre, QualWorld, Roche, Sobi and Takeda; personal fees as an invited speaker from AbbVie, AstraZeneca, BMS/Celgene, Gilead Kite, Incyte, Lilly, MSD, Novartis, Roche Pharma AG and Takeda; institutional funding from Esteve, MSD, Novartis and Takeda; and travel support from AbbVie, AstraZeneca, Gilead Kite, Lilly, MSD, Pierre Fabre, Roche, Takeda and Novartis. CBu reports personal fees for advisory board membership from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; personal fees as an invited speaker from AbbVie, BeiGene, Celltrion, Gilead Sciences, Incyte, Janssen, Lilly Deutschland GmbH, MorphoSys, Novartis, Pfizer, Regeneron, Roche and Sobi; and institutional funding from AbbVie Amgen, Bayer, Celltrion, Janssen, MSD, Pfizer and Roche (all for investigator-sponsored clinical trials and registries). MD reports personal fees as an advisory board member from AbbVie, AstraZeneca, BeiGene, BMS/Celgene, Gilead, Janssen, Lilly/Loxo, Novartis and Roche; personal fees as an invited speaker for AstraZeneca, BeiGene, Gilead/Kite, Janssen, Lilly, Novartis and Roche; institutional research grants from AbbVie, Bayer, Celgene, Janssen, Lilly and Roche; institutional funding from Gilead/Kite; and non-renumerated membership of the American Society of Clinical Oncology, American Society of Hematology (subcommittee), DGHO (prior Board member), EHA (Executive Board), ESMO (Faculty) and the Lymphoma Research Foundation (Mantle Cell Lymphoma Consortium). AD reports personal fees as an advisory board member for AbbVie, Acerta Pharma, AstraZeneca, BMS/Celgene, Genmab, Gilead, Incyte, Karyopharm, Kite Pharma, Regeneron, Roche, Sobi and Takeda; personal fees as an invited speaker for AstraZeneca, Gilead and Roche; institutional research grants for conduct of commercial research and funding of IST from Acerta Pharma and Roche; institutional research grants for conduct of commercial research from ADC Therapeutics, AstraZeneca, BMS/Celgene, Gilead and Pfizer; institutional research grant from MSD (no financial interest); non-renumerated leadership role, member and UK Board representative for the Precision Medicine in Aggressive Lymphoma Consortium of the International Extranodal Lymphoma Study Group; advisory role and international advisor for the Swiss SAKK Lymphoma Project Group and member of the UK National Cancer Research Institute's High Grade Lymphoma Study Group.
No external funding has been received for the preparation of this guideline. Production costs have been covered by ESMO (for Annals of Oncology) and EHA (for HemaSphere) central funds.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
