Tim Kinnaird MD, Sean Gallagher MD, Vasim Farooq PhD, Majd B. Protty PhD, Hannah Cranch MD, Peader Devlin MD, Andrew Sharp MD, Nick Curzen PhD, Peter Ludman MD, David Hildick-Smith MD, Tom Johnson PhD, Mamas A. Mamas DPhil
{"title":"针对无保护左主干疾病的临时PCI与计划PCI的院内预后:英国心血管介入协会数据库2006-2018年8574例病例分析。","authors":"Tim Kinnaird MD, Sean Gallagher MD, Vasim Farooq PhD, Majd B. Protty PhD, Hannah Cranch MD, Peader Devlin MD, Andrew Sharp MD, Nick Curzen PhD, Peter Ludman MD, David Hildick-Smith MD, Tom Johnson PhD, Mamas A. Mamas DPhil","doi":"10.1002/ccd.31210","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Although data suggests ad hoc percutaneous coronary intervention (PCI) results in similar patient outcomes compared to planned PCI in nonselected patients, data for ad hoc unprotected left main stem PCI (uLMS-PCI) are lacking.</p>\n </section>\n \n <section>\n \n <h3> Aim</h3>\n \n <p>To determine if in-hospital outcomes of uLMS-PCI vary by ad hoc versus planned basis.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Data were analyzed from all patients undergoing uLMS-PCI in the United Kingdom 2006–2018, and patients grouped into uLMS-PCI undertaken on an ad hoc or a planned basis. Patients who presented with ST-segment elevation, cardiogenic shock, or with an emergency PCI indication were excluded.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>In total, 8574 uLMS-PCI procedures were undertaken with 2837 (33.1%) of procedures performed on an ad hoc basis. There was a lower likelihood of intervention for stable angina (28.8% vs. 53.8%, <i>p</i> < 0.001) and a higher rate of potent P2Y12 inhibitor use (16.4% vs. 12.1%, <i>p</i> < 0.001) in the ad hoc PCI group compared to the planned PCI group. Patients undergoing uLMS-PCI on an ad hoc basis tended to undergo less complex procedures. Acute procedural complications including slow flow (odds ratio [OR]: 1.70, 95% confidence interval [CI]: 1.01–2.86), coronary dissection (OR: 1.41, 95% CI: 1.12–1.77) and shock induction (OR: 2.80, 95% CI: 1.64–4.78) were more likely in the ad hoc PCI group. In-hospital death (OR: 1.65, 95% CI: 1.19–2.27) and in-hospital major adverse cardiac or cerebrovascular events (OR: 1.50, 95% CI: 1.13–1.98) occurred more frequently in the ad hoc group. In sensitivity analyses, these observations did not differ when several subgroups were separately examined.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Ad hoc PCI for uLMS disease is associated with adverse outcomes compared to planned PCI. These data should inform uLMS-PCI procedural planning.</p>\n </section>\n </div>","PeriodicalId":9650,"journal":{"name":"Catheterization and Cardiovascular Interventions","volume":"104 4","pages":"697-706"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31210","citationCount":"0","resultStr":"{\"title\":\"In-hospital outcomes of ad hoc versus planned PCI for unprotected left-main disease: An analysis of 8574 cases from British Cardiovascular Intervention Society database 2006–2018\",\"authors\":\"Tim Kinnaird MD, Sean Gallagher MD, Vasim Farooq PhD, Majd B. Protty PhD, Hannah Cranch MD, Peader Devlin MD, Andrew Sharp MD, Nick Curzen PhD, Peter Ludman MD, David Hildick-Smith MD, Tom Johnson PhD, Mamas A. Mamas DPhil\",\"doi\":\"10.1002/ccd.31210\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Although data suggests ad hoc percutaneous coronary intervention (PCI) results in similar patient outcomes compared to planned PCI in nonselected patients, data for ad hoc unprotected left main stem PCI (uLMS-PCI) are lacking.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>To determine if in-hospital outcomes of uLMS-PCI vary by ad hoc versus planned basis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Data were analyzed from all patients undergoing uLMS-PCI in the United Kingdom 2006–2018, and patients grouped into uLMS-PCI undertaken on an ad hoc or a planned basis. Patients who presented with ST-segment elevation, cardiogenic shock, or with an emergency PCI indication were excluded.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>In total, 8574 uLMS-PCI procedures were undertaken with 2837 (33.1%) of procedures performed on an ad hoc basis. There was a lower likelihood of intervention for stable angina (28.8% vs. 53.8%, <i>p</i> < 0.001) and a higher rate of potent P2Y12 inhibitor use (16.4% vs. 12.1%, <i>p</i> < 0.001) in the ad hoc PCI group compared to the planned PCI group. Patients undergoing uLMS-PCI on an ad hoc basis tended to undergo less complex procedures. Acute procedural complications including slow flow (odds ratio [OR]: 1.70, 95% confidence interval [CI]: 1.01–2.86), coronary dissection (OR: 1.41, 95% CI: 1.12–1.77) and shock induction (OR: 2.80, 95% CI: 1.64–4.78) were more likely in the ad hoc PCI group. In-hospital death (OR: 1.65, 95% CI: 1.19–2.27) and in-hospital major adverse cardiac or cerebrovascular events (OR: 1.50, 95% CI: 1.13–1.98) occurred more frequently in the ad hoc group. In sensitivity analyses, these observations did not differ when several subgroups were separately examined.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Ad hoc PCI for uLMS disease is associated with adverse outcomes compared to planned PCI. These data should inform uLMS-PCI procedural planning.</p>\\n </section>\\n </div>\",\"PeriodicalId\":9650,\"journal\":{\"name\":\"Catheterization and Cardiovascular Interventions\",\"volume\":\"104 4\",\"pages\":\"697-706\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31210\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Catheterization and Cardiovascular Interventions\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31210\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Catheterization and Cardiovascular Interventions","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31210","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
In-hospital outcomes of ad hoc versus planned PCI for unprotected left-main disease: An analysis of 8574 cases from British Cardiovascular Intervention Society database 2006–2018
Background
Although data suggests ad hoc percutaneous coronary intervention (PCI) results in similar patient outcomes compared to planned PCI in nonselected patients, data for ad hoc unprotected left main stem PCI (uLMS-PCI) are lacking.
Aim
To determine if in-hospital outcomes of uLMS-PCI vary by ad hoc versus planned basis.
Methods
Data were analyzed from all patients undergoing uLMS-PCI in the United Kingdom 2006–2018, and patients grouped into uLMS-PCI undertaken on an ad hoc or a planned basis. Patients who presented with ST-segment elevation, cardiogenic shock, or with an emergency PCI indication were excluded.
Results
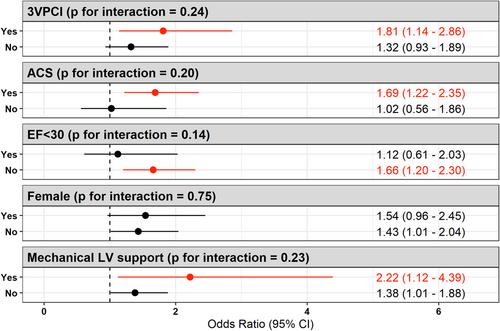
In total, 8574 uLMS-PCI procedures were undertaken with 2837 (33.1%) of procedures performed on an ad hoc basis. There was a lower likelihood of intervention for stable angina (28.8% vs. 53.8%, p < 0.001) and a higher rate of potent P2Y12 inhibitor use (16.4% vs. 12.1%, p < 0.001) in the ad hoc PCI group compared to the planned PCI group. Patients undergoing uLMS-PCI on an ad hoc basis tended to undergo less complex procedures. Acute procedural complications including slow flow (odds ratio [OR]: 1.70, 95% confidence interval [CI]: 1.01–2.86), coronary dissection (OR: 1.41, 95% CI: 1.12–1.77) and shock induction (OR: 2.80, 95% CI: 1.64–4.78) were more likely in the ad hoc PCI group. In-hospital death (OR: 1.65, 95% CI: 1.19–2.27) and in-hospital major adverse cardiac or cerebrovascular events (OR: 1.50, 95% CI: 1.13–1.98) occurred more frequently in the ad hoc group. In sensitivity analyses, these observations did not differ when several subgroups were separately examined.
Conclusions
Ad hoc PCI for uLMS disease is associated with adverse outcomes compared to planned PCI. These data should inform uLMS-PCI procedural planning.
期刊介绍:
Catheterization and Cardiovascular Interventions is an international journal covering the broad field of cardiovascular diseases. Subject material includes basic and clinical information that is derived from or related to invasive and interventional coronary or peripheral vascular techniques. The journal focuses on material that will be of immediate practical value to physicians providing patient care in the clinical laboratory setting. To accomplish this, the journal publishes Preliminary Reports and Work In Progress articles that complement the traditional Original Studies, Case Reports, and Comprehensive Reviews. Perspective and insight concerning controversial subjects and evolving technologies are provided regularly through Editorial Commentaries furnished by members of the Editorial Board and other experts. Articles are subject to double-blind peer review and complete editorial evaluation prior to any decision regarding acceptability.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
