Natascha Majunke, Dan Philipp, Lorenz Weidhase, Bastian Pasieka, Kevin Kunz, Frank Seidel, Robert Scharm, Sirak Petros
{"title":"重症内科病人的被动抬腿试验与快速输液挑战。","authors":"Natascha Majunke, Dan Philipp, Lorenz Weidhase, Bastian Pasieka, Kevin Kunz, Frank Seidel, Robert Scharm, Sirak Petros","doi":"10.1007/s00063-024-01176-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The passive leg raising (PLR) test is a simple test to detect preload responsiveness. However, variable fluid doses and infusion times were used in studies evaluating the effect of PLR. Studies showed that the effect of fluid challenge on hemodynamics dissipates in 10 min. This prospective study aimed to compare PLR and a rapid fluid challenge (RFC) with a 300-ml bolus infused within 5 min in adult patients with a hemodynamic compromise.</p><p><strong>Materials and methods: </strong>Critically ill medical patients with signs of systemic hypoperfusion were included if volume expansion was considered. Hemodynamic status was assessed with continuous measurements of cardiac output (CO), when possible, and mean arterial pressure (MAP) at baseline, during PLR, and after RFC.</p><p><strong>Results: </strong>A total of 124 patients with a median age of 65.0 years were included. Their acute physiology and chronic health evaluation (APACHE) II score was 19.7 ± 6.0, with a sequential organ failure assessment (SOFA) score of 9.0 ± 4.4. Sepsis was diagnosed in 73.3%, and 79.8% of the patients were already receiving a norepinephrine infusion. Invasive MAP monitoring was established in all patients, while continuous CO recording was possible in 42 patients (33.9%). Based on CO changes, compared with those with RFC, the false positive and false negative rates with PLR were 21.7 and 36.8%, respectively, with positive and negative predictive values of 70.6 and 72.0%, respectively. Based on MAP changes, compared with those with RFC, the false positive and false negative rates with PLR compared to RFC were 38.2% and 43.3%, respectively, with positive and negative predictive values of 64.4 and 54.0%, respectively.</p><p><strong>Conclusion: </strong>This study demonstrated a moderate agreement between PLR and RFC in hemodynamically compromised medical patients, which should be considered when testing preload responsiveness.</p>","PeriodicalId":49019,"journal":{"name":"Medizinische Klinik-Intensivmedizin Und Notfallmedizin","volume":" ","pages":"316-321"},"PeriodicalIF":1.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12040970/pdf/","citationCount":"0","resultStr":"{\"title\":\"Passive leg raising test versus rapid fluid challenge in critically ill medical patients.\",\"authors\":\"Natascha Majunke, Dan Philipp, Lorenz Weidhase, Bastian Pasieka, Kevin Kunz, Frank Seidel, Robert Scharm, Sirak Petros\",\"doi\":\"10.1007/s00063-024-01176-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The passive leg raising (PLR) test is a simple test to detect preload responsiveness. However, variable fluid doses and infusion times were used in studies evaluating the effect of PLR. Studies showed that the effect of fluid challenge on hemodynamics dissipates in 10 min. This prospective study aimed to compare PLR and a rapid fluid challenge (RFC) with a 300-ml bolus infused within 5 min in adult patients with a hemodynamic compromise.</p><p><strong>Materials and methods: </strong>Critically ill medical patients with signs of systemic hypoperfusion were included if volume expansion was considered. Hemodynamic status was assessed with continuous measurements of cardiac output (CO), when possible, and mean arterial pressure (MAP) at baseline, during PLR, and after RFC.</p><p><strong>Results: </strong>A total of 124 patients with a median age of 65.0 years were included. Their acute physiology and chronic health evaluation (APACHE) II score was 19.7 ± 6.0, with a sequential organ failure assessment (SOFA) score of 9.0 ± 4.4. Sepsis was diagnosed in 73.3%, and 79.8% of the patients were already receiving a norepinephrine infusion. Invasive MAP monitoring was established in all patients, while continuous CO recording was possible in 42 patients (33.9%). Based on CO changes, compared with those with RFC, the false positive and false negative rates with PLR were 21.7 and 36.8%, respectively, with positive and negative predictive values of 70.6 and 72.0%, respectively. Based on MAP changes, compared with those with RFC, the false positive and false negative rates with PLR compared to RFC were 38.2% and 43.3%, respectively, with positive and negative predictive values of 64.4 and 54.0%, respectively.</p><p><strong>Conclusion: </strong>This study demonstrated a moderate agreement between PLR and RFC in hemodynamically compromised medical patients, which should be considered when testing preload responsiveness.</p>\",\"PeriodicalId\":49019,\"journal\":{\"name\":\"Medizinische Klinik-Intensivmedizin Und Notfallmedizin\",\"volume\":\" \",\"pages\":\"316-321\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12040970/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medizinische Klinik-Intensivmedizin Und Notfallmedizin\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00063-024-01176-2\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medizinische Klinik-Intensivmedizin Und Notfallmedizin","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00063-024-01176-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/6 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Passive leg raising test versus rapid fluid challenge in critically ill medical patients.
Background: The passive leg raising (PLR) test is a simple test to detect preload responsiveness. However, variable fluid doses and infusion times were used in studies evaluating the effect of PLR. Studies showed that the effect of fluid challenge on hemodynamics dissipates in 10 min. This prospective study aimed to compare PLR and a rapid fluid challenge (RFC) with a 300-ml bolus infused within 5 min in adult patients with a hemodynamic compromise.
Materials and methods: Critically ill medical patients with signs of systemic hypoperfusion were included if volume expansion was considered. Hemodynamic status was assessed with continuous measurements of cardiac output (CO), when possible, and mean arterial pressure (MAP) at baseline, during PLR, and after RFC.
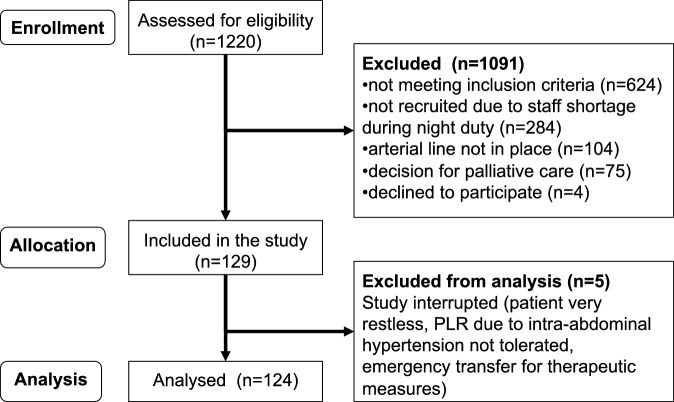
Results: A total of 124 patients with a median age of 65.0 years were included. Their acute physiology and chronic health evaluation (APACHE) II score was 19.7 ± 6.0, with a sequential organ failure assessment (SOFA) score of 9.0 ± 4.4. Sepsis was diagnosed in 73.3%, and 79.8% of the patients were already receiving a norepinephrine infusion. Invasive MAP monitoring was established in all patients, while continuous CO recording was possible in 42 patients (33.9%). Based on CO changes, compared with those with RFC, the false positive and false negative rates with PLR were 21.7 and 36.8%, respectively, with positive and negative predictive values of 70.6 and 72.0%, respectively. Based on MAP changes, compared with those with RFC, the false positive and false negative rates with PLR compared to RFC were 38.2% and 43.3%, respectively, with positive and negative predictive values of 64.4 and 54.0%, respectively.
Conclusion: This study demonstrated a moderate agreement between PLR and RFC in hemodynamically compromised medical patients, which should be considered when testing preload responsiveness.
期刊介绍:
Medizinische Klinik – Intensivmedizin und Notfallmedizin is an internationally respected interdisciplinary journal. It is intended for physicians, nurses, respiratory and physical therapists active in intensive care and accident/emergency units, but also for internists, anesthesiologists, surgeons, neurologists, and pediatricians with special interest in intensive care medicine.
Comprehensive reviews describe the most recent advances in the field of internal medicine with special focus on intensive care problems. Freely submitted original articles present important studies in this discipline and promote scientific exchange, while articles in the category Photo essay feature interesting cases and aim at optimizing diagnostic and therapeutic strategies. In the rubric journal club well-respected experts comment on outstanding international publications. Review articles under the rubric "Continuing Medical Education" present verified results of scientific research and their integration into daily practice. The rubrics "Nursing practice" and "Physical therapy" round out the information.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
