{"title":"血糖控制是糖尿病患者肝细胞癌和肝脏相关死亡率的一个可改变的风险因素","authors":"Xianhua Mao, Ka-Shing Cheung, Jing-Tong Tan, Lung-Yi Mak, Chi-Ho Lee, Chi-Leung Chiang, Ho-Ming Cheng, Rex Wan-Hin Hui, Wai K. Leung, Man-Fung Yuen, Wai-Kay Seto","doi":"10.1111/apt.18254","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Optimal glycaemic control has well-established health benefits in patients with diabetes mellitus (DM). It is uncertain whether optimal glycaemic control can benefit liver-related outcomes.</p>\n </section>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>To examine the association of optimal glycaemic control with hepatocellular carcinoma (HCC) and liver-related mortality.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In a population-based cohort, we identified patients with newly diagnosed DM between 2001 and 2016 in Hong Kong. Optimal glycaemic control was defined as mean haemoglobin A1c (HbA1c) <7% during the 3-year lead-in period after DM diagnosis. By applying propensity score matching to balance covariates, we analysed glycaemic control via competing risk models with outcomes of interest being HCC and liver-related mortality.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We identified 146,430 patients (52.2% males, mean age 61.4 ± 11.8 years). During a median follow-up duration of 7.0 years, 1099 (0.8%) and 978 (0.7%) patients developed HCC and liver-related deaths. Optimal glycaemic control, when compared to suboptimal glycaemic control, was associated with reduced risk of HCC (subdistribution hazard ratio [SHR] 0.70, 95% CI 0.61–0.79). The risk of HCC increased with incremental HbA1c increases beyond >7% (SHR 1.29–1.71). Significant associations with HCC were also found irrespective of age (SHR 0.54–0.80), sex (SHR 0.68–0.69), BMI <25 or ≥25 kg/m<sup>2</sup> (SHR 0.63–0.75), smoking (SHR 0.61–0.72), hepatic steatosis (SHR 0.67–0.68) and aspirin/statin/metformin use (SHR 0.67–0.75). A lower risk of liver-related mortality in relation to optimal glycaemic control was also observed (SHR 0.70, 95% CI 0.61–0.80).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Glycaemic control is an independent risk factor for HCC and liver-related mortality, and should be incorporated into oncoprotective strategies in the general DM population.</p>\n </section>\n </div>","PeriodicalId":121,"journal":{"name":"Alimentary Pharmacology & Therapeutics","volume":"60 10","pages":"1398-1408"},"PeriodicalIF":6.7000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/apt.18254","citationCount":"0","resultStr":"{\"title\":\"Glycaemic control is a modifiable risk factor for hepatocellular carcinoma and liver-related mortality in patients with diabetes\",\"authors\":\"Xianhua Mao, Ka-Shing Cheung, Jing-Tong Tan, Lung-Yi Mak, Chi-Ho Lee, Chi-Leung Chiang, Ho-Ming Cheng, Rex Wan-Hin Hui, Wai K. Leung, Man-Fung Yuen, Wai-Kay Seto\",\"doi\":\"10.1111/apt.18254\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Optimal glycaemic control has well-established health benefits in patients with diabetes mellitus (DM). It is uncertain whether optimal glycaemic control can benefit liver-related outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>To examine the association of optimal glycaemic control with hepatocellular carcinoma (HCC) and liver-related mortality.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>In a population-based cohort, we identified patients with newly diagnosed DM between 2001 and 2016 in Hong Kong. Optimal glycaemic control was defined as mean haemoglobin A1c (HbA1c) <7% during the 3-year lead-in period after DM diagnosis. By applying propensity score matching to balance covariates, we analysed glycaemic control via competing risk models with outcomes of interest being HCC and liver-related mortality.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We identified 146,430 patients (52.2% males, mean age 61.4 ± 11.8 years). During a median follow-up duration of 7.0 years, 1099 (0.8%) and 978 (0.7%) patients developed HCC and liver-related deaths. Optimal glycaemic control, when compared to suboptimal glycaemic control, was associated with reduced risk of HCC (subdistribution hazard ratio [SHR] 0.70, 95% CI 0.61–0.79). The risk of HCC increased with incremental HbA1c increases beyond >7% (SHR 1.29–1.71). Significant associations with HCC were also found irrespective of age (SHR 0.54–0.80), sex (SHR 0.68–0.69), BMI <25 or ≥25 kg/m<sup>2</sup> (SHR 0.63–0.75), smoking (SHR 0.61–0.72), hepatic steatosis (SHR 0.67–0.68) and aspirin/statin/metformin use (SHR 0.67–0.75). A lower risk of liver-related mortality in relation to optimal glycaemic control was also observed (SHR 0.70, 95% CI 0.61–0.80).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Glycaemic control is an independent risk factor for HCC and liver-related mortality, and should be incorporated into oncoprotective strategies in the general DM population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":121,\"journal\":{\"name\":\"Alimentary Pharmacology & Therapeutics\",\"volume\":\"60 10\",\"pages\":\"1398-1408\"},\"PeriodicalIF\":6.7000,\"publicationDate\":\"2024-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/apt.18254\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Alimentary Pharmacology & Therapeutics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/apt.18254\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Alimentary Pharmacology & Therapeutics","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/apt.18254","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Glycaemic control is a modifiable risk factor for hepatocellular carcinoma and liver-related mortality in patients with diabetes
Background
Optimal glycaemic control has well-established health benefits in patients with diabetes mellitus (DM). It is uncertain whether optimal glycaemic control can benefit liver-related outcomes.
Aims
To examine the association of optimal glycaemic control with hepatocellular carcinoma (HCC) and liver-related mortality.
Methods
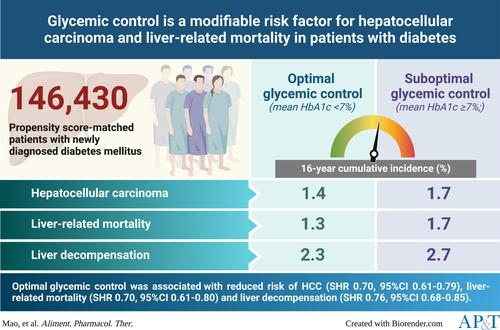
In a population-based cohort, we identified patients with newly diagnosed DM between 2001 and 2016 in Hong Kong. Optimal glycaemic control was defined as mean haemoglobin A1c (HbA1c) <7% during the 3-year lead-in period after DM diagnosis. By applying propensity score matching to balance covariates, we analysed glycaemic control via competing risk models with outcomes of interest being HCC and liver-related mortality.
Results
We identified 146,430 patients (52.2% males, mean age 61.4 ± 11.8 years). During a median follow-up duration of 7.0 years, 1099 (0.8%) and 978 (0.7%) patients developed HCC and liver-related deaths. Optimal glycaemic control, when compared to suboptimal glycaemic control, was associated with reduced risk of HCC (subdistribution hazard ratio [SHR] 0.70, 95% CI 0.61–0.79). The risk of HCC increased with incremental HbA1c increases beyond >7% (SHR 1.29–1.71). Significant associations with HCC were also found irrespective of age (SHR 0.54–0.80), sex (SHR 0.68–0.69), BMI <25 or ≥25 kg/m2 (SHR 0.63–0.75), smoking (SHR 0.61–0.72), hepatic steatosis (SHR 0.67–0.68) and aspirin/statin/metformin use (SHR 0.67–0.75). A lower risk of liver-related mortality in relation to optimal glycaemic control was also observed (SHR 0.70, 95% CI 0.61–0.80).
Conclusions
Glycaemic control is an independent risk factor for HCC and liver-related mortality, and should be incorporated into oncoprotective strategies in the general DM population.
期刊介绍:
Alimentary Pharmacology & Therapeutics is a global pharmacology journal focused on the impact of drugs on the human gastrointestinal and hepato-biliary systems. It covers a diverse range of topics, often with immediate clinical relevance to its readership.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
