Talha Badar, Ravi Narra, Alice S. Mims, Michael G. Heckman, Rory M. Shallis, Sheikh Fahad, Cameron Hunter, Vamsi Kota, Tamer Adel Othman, Brian Jonas, Shreya Desai, Guilherme Sacchi de Camargo Correia, Anand Patel, Adam S. DuVall, Neil Palmisiano, Emily Curran, Zulfa Omer, Anjali Advani, Ehab Atallah, Mark Litzow
{"title":"诱导方案强度和异体干细胞移植对费城染色体阳性急性淋巴细胞白血病患者存活率的影响:一项多机构研究","authors":"Talha Badar, Ravi Narra, Alice S. Mims, Michael G. Heckman, Rory M. Shallis, Sheikh Fahad, Cameron Hunter, Vamsi Kota, Tamer Adel Othman, Brian Jonas, Shreya Desai, Guilherme Sacchi de Camargo Correia, Anand Patel, Adam S. DuVall, Neil Palmisiano, Emily Curran, Zulfa Omer, Anjali Advani, Ehab Atallah, Mark Litzow","doi":"10.1002/ajh.27475","DOIUrl":null,"url":null,"abstract":"<p>\n </p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 12","pages":"2388-2391"},"PeriodicalIF":9.9000,"publicationDate":"2024-09-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27475","citationCount":"0","resultStr":"{\"title\":\"Impact of induction regimens intensity and allogeneic stem cell transplantation on survival of patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: A multi-institutional study\",\"authors\":\"Talha Badar, Ravi Narra, Alice S. Mims, Michael G. Heckman, Rory M. Shallis, Sheikh Fahad, Cameron Hunter, Vamsi Kota, Tamer Adel Othman, Brian Jonas, Shreya Desai, Guilherme Sacchi de Camargo Correia, Anand Patel, Adam S. DuVall, Neil Palmisiano, Emily Curran, Zulfa Omer, Anjali Advani, Ehab Atallah, Mark Litzow\",\"doi\":\"10.1002/ajh.27475\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>\\n </p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"99 12\",\"pages\":\"2388-2391\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-09-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27475\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27475\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27475","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
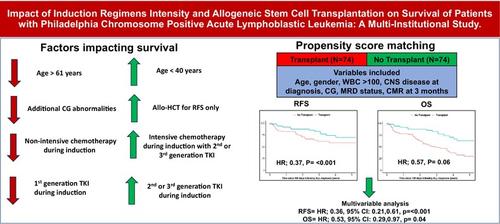
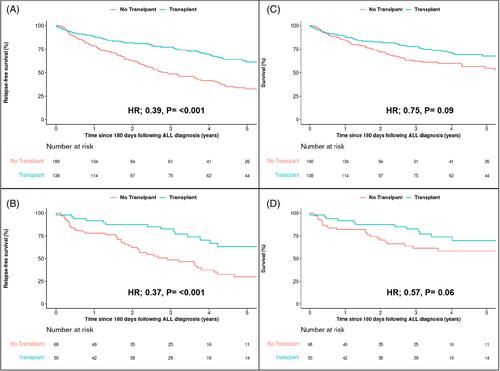
37, p = <.001)(图1B)。图1在图形浏览器中打开PowerPoint接受和未接受同种异体干细胞移植(allo-HCT)的存活率。(A)诊断后180天基线时间点后的RFS,(B)倾向得分匹配队列中异体干细胞移植180天后的RFS,(C)诊断后180天基线时间点后的OS,(D)倾向得分匹配队列中异体干细胞移植180天后的OS。在对补充表 4 中强调的变量进行调整后,我们比较了倾向分数匹配的同种异体肝移植和非同种异体肝移植患者的结果。在未调整分析(HR;0.37,p = <;.001,图 1C)和多变量分析(HR;0.36,p = <;.001)中,同种异体肝移植患者的无复发生存期均优于非同种异体肝移植患者,见补充表 5。在OS的多变量分析中,观察到与诊断时的年龄(HR [年龄>61岁 vs. ≤40岁];2.89,p <.001)和诱导期间使用的TKI类型(HR [第2代/第3代 vs. 第1代];0.66,p = .02)显著相关,补充表6。同样,OS 与 MFC-MRD 阴性之间也没有发现明显的关联(HR 1.12,p = .56,补图 2C)。虽然我们在未调整分析中观察到CMR对OS的益处(补充图2D),但在多变量分析中却没有保留(HR 0.90,p = .55)(补充表3)。根据3个月时达到CMR(HR;0.87,p = .59)或未达到CMR(HR;0.48,p = .11),异体血细胞移植对OS没有显著影响。在 180 天时间点(HR;0.75,p = .09,图 1C)或使用倾向匹配评分后(HR;0.57,p = .06(图 1D)),我们没有观察到异体肝移植对 OS 有明显改善。在我们的多中心真实世界分析中,在调整了混杂变量后,我们观察到诊断时年龄较大(>61 岁 vs. ≤ 40 岁)、诱导时使用第一代 TKI vs. 第二代/第三代 TKI 的患者的 RFS 和 OS 明显较差。在多变量分析中,治疗方案强度(NIC与IC)似乎对RFS或OS没有显著影响。同种异体干细胞移植有益于改善RFS,但对3个月时达到CMR的患者的OS无益。BCR::ABL1导向的TKI的出现和纳入一线方案改善了Ph+ ALL患者的生存。与单独化疗相比,所有TKI与化疗的联合用药都能提高生存率,但第二代或第三代TKI的获益最大,其OS更长,耐药突变更少。2 波纳替尼是最有效的BCR::ABL1导向TKI之一,对野生型和突变型ABL1均有效,尤其是T315I突变。最近,一项针对Ph+ ALL的III期研究评估了波那替尼与伊马替尼及NIC的疗效,结果显示波那替尼的MRD阴性CR率更优,无事件生存期也有改善趋势。在我们的分析中,我们观察到,与伊马替尼相比,以第二代或第三代 TKI 为基础的前线治疗组合可显著改善 RFS 和 OS,这与之前的观察结果一致。几项NIC+TKI联合治疗的前瞻性研究显示,良好的CR率在90%-95%之间;然而,长期生存率仍然不高,在35%-45%之间。然而,由于更好的耐受性和疗效,先期使用 blinatumomab + TKI 的无化疗诱导疗法正逐渐受到青睐,6 目前正在对其与 IC + TKI 联合疗法进行随机评估。在最近进行的回顾性分析中,我们分析了230例Ph+ ALL患者,这些患者在确诊90天后进行了CMR,以研究allo-HCT是否能有效改善OS.4 研究显示,allo-HCT能有效降低累积复发率,但对改善OS没有影响。与这些观察结果类似,我们也观察到,无论 3 个月时是否达到 CMR,allo-HCT 对改善 RFS 都有良好影响,但对 OS 却没有影响。然而,经过倾向评分匹配和多变量分析后,我们确实发现allo-HCT对改善RFS和OS有好处。我们承认我们的分析存在局限性,数据存在异质性,倾向得分匹配组的样本量相对较小,因此可能存在 II 型误差(即:allo-HCST 在改善 RFS 和 OS 方面的益处)。
Impact of induction regimens intensity and allogeneic stem cell transplantation on survival of patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: A multi-institutional study
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
