Maria A. Pabon, Muthiah Vaduganathan, Brian L. Claggett, Safia Chatur, Sara Siqueira, Pablo Marti-Castellote, Rudolf A. de Boer, Adrian F. Hernandez, Silvio E. Inzucchi, Mikhail N. Kosiborod, Carolyn S.P. Lam, Felipe Martinez, Sanjiv J. Shah, Akshay S. Desai, Pardeep S. Jhund, John J.V. McMurray, Scott D. Solomon, Orly Vardeny
{"title":"DELIVER 试验中射血分数改善型心力衰竭患者的住院治疗过程","authors":"Maria A. Pabon, Muthiah Vaduganathan, Brian L. Claggett, Safia Chatur, Sara Siqueira, Pablo Marti-Castellote, Rudolf A. de Boer, Adrian F. Hernandez, Silvio E. Inzucchi, Mikhail N. Kosiborod, Carolyn S.P. Lam, Felipe Martinez, Sanjiv J. Shah, Akshay S. Desai, Pardeep S. Jhund, John J.V. McMurray, Scott D. Solomon, Orly Vardeny","doi":"10.1002/ejhf.3410","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>Patients with heart failure (HF) with improved ejection fraction (HFimpEF) may face residual risks of clinical events that are comparable to those experienced by patients with HF whose left ventricular ejection fraction (LVEF) has consistently been above 40%. However, little is known about the clinical course of patients with HFimpEF during hospitalization for HF.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>DELIVER randomized patients with HF and LVEF >40% to dapagliflozin or placebo, including HFimpEF (LVEF previously ≤40%). We evaluated all HF hospitalizations adjudicated by the clinical endpoints committee with available data for determination of in-hospital course. Complicated hospitalization was defined as any hospitalization requiring intensive care unit stay, intravenous vasopressors/inotropes/vasodilators, invasive or non-invasive ventilation, mechanical fluid removal, ultrafiltration, or mechanical circulatory support. LVEF changes were extracted using a validated GPT-3.5, a large language model, via a secure private endpoint. Of the 6263 patients enrolled in DELIVER, 1151 (18%) had HFimpEF. During a median follow-up of 2.3 years, there were 224 total HF hospitalizations in 144 patients with HFimpEF and 985 in 603 patients with LVEF consistently >40%. Patients with HFimpEF experienced higher rates of complicated HF hospitalization as compared with patients with LVEF consistently >40% (39% vs. 27%; <i>p</i> < 0.001). Among those who experienced a first HF hospitalization, there was no significant difference in length of stay or in-hospital mortality between patients with HFimpEF versus LVEF consistently >40%. In a subset of participants who had at least one LVEF measurement available during HF hospitalization, 66% of those with HFimpEF and 29% of patients with LVEF consistently >40% experienced a reduction in their LVEF to ≤40% from the time of enrolment (<i>p</i> < 0.001). In the entire DELIVER cohort, dapagliflozin reduced total uncomplicated and complicated HF hospitalizations, irrespective of HFimpEF status (<i>p</i><sub>interaction</sub> ≥0.30).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Among patients hospitalized for HF in DELIVER, those with HFimpEF experienced a more adverse in-hospital clinical course, necessitating higher resource utilization beyond standard diuretic therapy compared with patients with HF and LVEF consistently >40%, but had similar in-hospital mortality. Treatment benefits of dapagliflozin were not modified by hospitalization type.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"26 12","pages":"2532-2540"},"PeriodicalIF":10.8000,"publicationDate":"2024-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3410","citationCount":"0","resultStr":"{\"title\":\"In-hospital course of patients with heart failure with improved ejection fraction in the DELIVER trial\",\"authors\":\"Maria A. Pabon, Muthiah Vaduganathan, Brian L. Claggett, Safia Chatur, Sara Siqueira, Pablo Marti-Castellote, Rudolf A. de Boer, Adrian F. Hernandez, Silvio E. Inzucchi, Mikhail N. Kosiborod, Carolyn S.P. Lam, Felipe Martinez, Sanjiv J. Shah, Akshay S. Desai, Pardeep S. Jhund, John J.V. McMurray, Scott D. Solomon, Orly Vardeny\",\"doi\":\"10.1002/ejhf.3410\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Patients with heart failure (HF) with improved ejection fraction (HFimpEF) may face residual risks of clinical events that are comparable to those experienced by patients with HF whose left ventricular ejection fraction (LVEF) has consistently been above 40%. However, little is known about the clinical course of patients with HFimpEF during hospitalization for HF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>DELIVER randomized patients with HF and LVEF >40% to dapagliflozin or placebo, including HFimpEF (LVEF previously ≤40%). We evaluated all HF hospitalizations adjudicated by the clinical endpoints committee with available data for determination of in-hospital course. Complicated hospitalization was defined as any hospitalization requiring intensive care unit stay, intravenous vasopressors/inotropes/vasodilators, invasive or non-invasive ventilation, mechanical fluid removal, ultrafiltration, or mechanical circulatory support. LVEF changes were extracted using a validated GPT-3.5, a large language model, via a secure private endpoint. Of the 6263 patients enrolled in DELIVER, 1151 (18%) had HFimpEF. During a median follow-up of 2.3 years, there were 224 total HF hospitalizations in 144 patients with HFimpEF and 985 in 603 patients with LVEF consistently >40%. Patients with HFimpEF experienced higher rates of complicated HF hospitalization as compared with patients with LVEF consistently >40% (39% vs. 27%; <i>p</i> < 0.001). Among those who experienced a first HF hospitalization, there was no significant difference in length of stay or in-hospital mortality between patients with HFimpEF versus LVEF consistently >40%. In a subset of participants who had at least one LVEF measurement available during HF hospitalization, 66% of those with HFimpEF and 29% of patients with LVEF consistently >40% experienced a reduction in their LVEF to ≤40% from the time of enrolment (<i>p</i> < 0.001). In the entire DELIVER cohort, dapagliflozin reduced total uncomplicated and complicated HF hospitalizations, irrespective of HFimpEF status (<i>p</i><sub>interaction</sub> ≥0.30).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Among patients hospitalized for HF in DELIVER, those with HFimpEF experienced a more adverse in-hospital clinical course, necessitating higher resource utilization beyond standard diuretic therapy compared with patients with HF and LVEF consistently >40%, but had similar in-hospital mortality. Treatment benefits of dapagliflozin were not modified by hospitalization type.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"26 12\",\"pages\":\"2532-2540\"},\"PeriodicalIF\":10.8000,\"publicationDate\":\"2024-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3410\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3410\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3410","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
In-hospital course of patients with heart failure with improved ejection fraction in the DELIVER trial
Aims
Patients with heart failure (HF) with improved ejection fraction (HFimpEF) may face residual risks of clinical events that are comparable to those experienced by patients with HF whose left ventricular ejection fraction (LVEF) has consistently been above 40%. However, little is known about the clinical course of patients with HFimpEF during hospitalization for HF.
Methods and results
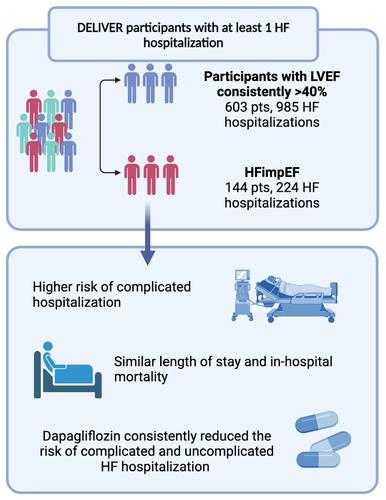
DELIVER randomized patients with HF and LVEF >40% to dapagliflozin or placebo, including HFimpEF (LVEF previously ≤40%). We evaluated all HF hospitalizations adjudicated by the clinical endpoints committee with available data for determination of in-hospital course. Complicated hospitalization was defined as any hospitalization requiring intensive care unit stay, intravenous vasopressors/inotropes/vasodilators, invasive or non-invasive ventilation, mechanical fluid removal, ultrafiltration, or mechanical circulatory support. LVEF changes were extracted using a validated GPT-3.5, a large language model, via a secure private endpoint. Of the 6263 patients enrolled in DELIVER, 1151 (18%) had HFimpEF. During a median follow-up of 2.3 years, there were 224 total HF hospitalizations in 144 patients with HFimpEF and 985 in 603 patients with LVEF consistently >40%. Patients with HFimpEF experienced higher rates of complicated HF hospitalization as compared with patients with LVEF consistently >40% (39% vs. 27%; p < 0.001). Among those who experienced a first HF hospitalization, there was no significant difference in length of stay or in-hospital mortality between patients with HFimpEF versus LVEF consistently >40%. In a subset of participants who had at least one LVEF measurement available during HF hospitalization, 66% of those with HFimpEF and 29% of patients with LVEF consistently >40% experienced a reduction in their LVEF to ≤40% from the time of enrolment (p < 0.001). In the entire DELIVER cohort, dapagliflozin reduced total uncomplicated and complicated HF hospitalizations, irrespective of HFimpEF status (pinteraction ≥0.30).
Conclusions
Among patients hospitalized for HF in DELIVER, those with HFimpEF experienced a more adverse in-hospital clinical course, necessitating higher resource utilization beyond standard diuretic therapy compared with patients with HF and LVEF consistently >40%, but had similar in-hospital mortality. Treatment benefits of dapagliflozin were not modified by hospitalization type.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
