Michelle S Rockwell, Brianna Chang, Vivian Zagarese, Jamie K Turner, Ally Southworth, YingXing Wu, Paul Yeaton, Li Li, Jeffrey S Stein, Sarah H Parker, John W Epling
{"title":"患者在癌症筛查过程中的 \"淤积\"(行政负担)体验及其与筛查完成度、体验和对医疗系统的不信任之间的关系。","authors":"Michelle S Rockwell, Brianna Chang, Vivian Zagarese, Jamie K Turner, Ally Southworth, YingXing Wu, Paul Yeaton, Li Li, Jeffrey S Stein, Sarah H Parker, John W Epling","doi":"10.1136/fmch-2024-002933","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>'Sludge' refers to administrative burdens or frictions that preclude people from getting what they want or need (eg, duplicative forms, complicated instructions, long waiting times). This mixed methods study evaluated patients' perceptions of sludge in the colorectal cancer (CRC) screening process and some impacts of this sludge.</p><p><strong>Design: </strong>We employed an exploratory sequential mixed methods study design that comprised patient interviews and a patient survey. The interviews informed final survey revisions and captured contextual data about patients' experiences with sludge. Interview transcripts were inductively and deductively analysed to identify overarching themes. The survey quantified sludge, delayed or forgone screenings, screening experience (Net Promoter Score) and health system distrust (Health System Distrust Scale). We used χ<sup>2</sup> or t-tests for univariable comparisons and logistic or linear regressions to evaluate the association between cumulative sludge score and delayed or forgone screenings, screening experience and health system distrust. Results were integrated for interpretation.</p><p><strong>Setting: </strong>Southeastern United States.</p><p><strong>Participants: </strong>Patients who were 45-75 years of age, at average risk for CRC and had either completed or been referred for CRC screening (colonoscopy or stool-based test) within the previous 12 months.</p><p><strong>Results: </strong>22 interview participants and 255 survey participants completed the study. 38 (15%) survey participants rated their screening experience as poor (Net Promoter Score=0-7 out of 10). The mean (SD) Health System Distrust Scale score was 22.4 (6.3) out of 45 possible points (higher score=greater distrust). Perceptions of sludge in the CRC screening process varied, with long waiting times and burdensome communication being the most common sources (58% and 35% of participants, respectively). Sludge was positively associated with delayed or forgone screenings (OR=1.42, 95% CI 1.28, 1.57, p<0.001), poor screening experience (OR=1.15, 95% CI 1.04, 1.28, p=0.009) and health system distrust (β=0.47, p<0.001). Qualitative findings add descriptive detail about sludge encountered, context to impacts experienced, and illustrate the heavy emotional impact of sludge: '<i>it just isn't worth it'</i>.</p><p><strong>Conclusion: </strong>Efforts to reduce sludge in the CRC screening process may improve timely completion of CRC screening, enhance patient experience and restore trust in the health system.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"12 Suppl 2","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664340/pdf/","citationCount":"0","resultStr":"{\"title\":\"Patients' experiences with 'sludge' (administrative burden) in the cancer screening process and its relationship with screening completion, experience and health system distrust.\",\"authors\":\"Michelle S Rockwell, Brianna Chang, Vivian Zagarese, Jamie K Turner, Ally Southworth, YingXing Wu, Paul Yeaton, Li Li, Jeffrey S Stein, Sarah H Parker, John W Epling\",\"doi\":\"10.1136/fmch-2024-002933\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>'Sludge' refers to administrative burdens or frictions that preclude people from getting what they want or need (eg, duplicative forms, complicated instructions, long waiting times). This mixed methods study evaluated patients' perceptions of sludge in the colorectal cancer (CRC) screening process and some impacts of this sludge.</p><p><strong>Design: </strong>We employed an exploratory sequential mixed methods study design that comprised patient interviews and a patient survey. The interviews informed final survey revisions and captured contextual data about patients' experiences with sludge. Interview transcripts were inductively and deductively analysed to identify overarching themes. The survey quantified sludge, delayed or forgone screenings, screening experience (Net Promoter Score) and health system distrust (Health System Distrust Scale). We used χ<sup>2</sup> or t-tests for univariable comparisons and logistic or linear regressions to evaluate the association between cumulative sludge score and delayed or forgone screenings, screening experience and health system distrust. Results were integrated for interpretation.</p><p><strong>Setting: </strong>Southeastern United States.</p><p><strong>Participants: </strong>Patients who were 45-75 years of age, at average risk for CRC and had either completed or been referred for CRC screening (colonoscopy or stool-based test) within the previous 12 months.</p><p><strong>Results: </strong>22 interview participants and 255 survey participants completed the study. 38 (15%) survey participants rated their screening experience as poor (Net Promoter Score=0-7 out of 10). The mean (SD) Health System Distrust Scale score was 22.4 (6.3) out of 45 possible points (higher score=greater distrust). Perceptions of sludge in the CRC screening process varied, with long waiting times and burdensome communication being the most common sources (58% and 35% of participants, respectively). Sludge was positively associated with delayed or forgone screenings (OR=1.42, 95% CI 1.28, 1.57, p<0.001), poor screening experience (OR=1.15, 95% CI 1.04, 1.28, p=0.009) and health system distrust (β=0.47, p<0.001). Qualitative findings add descriptive detail about sludge encountered, context to impacts experienced, and illustrate the heavy emotional impact of sludge: '<i>it just isn't worth it'</i>.</p><p><strong>Conclusion: </strong>Efforts to reduce sludge in the CRC screening process may improve timely completion of CRC screening, enhance patient experience and restore trust in the health system.</p>\",\"PeriodicalId\":44590,\"journal\":{\"name\":\"Family Medicine and Community Health\",\"volume\":\"12 Suppl 2\",\"pages\":\"\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11664340/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Family Medicine and Community Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/fmch-2024-002933\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2024-002933","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Patients' experiences with 'sludge' (administrative burden) in the cancer screening process and its relationship with screening completion, experience and health system distrust.
Objective: 'Sludge' refers to administrative burdens or frictions that preclude people from getting what they want or need (eg, duplicative forms, complicated instructions, long waiting times). This mixed methods study evaluated patients' perceptions of sludge in the colorectal cancer (CRC) screening process and some impacts of this sludge.
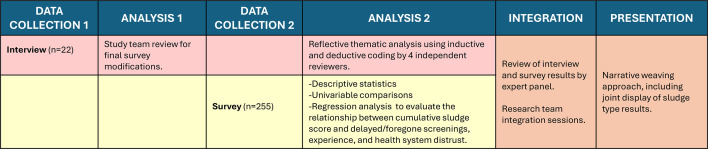
Design: We employed an exploratory sequential mixed methods study design that comprised patient interviews and a patient survey. The interviews informed final survey revisions and captured contextual data about patients' experiences with sludge. Interview transcripts were inductively and deductively analysed to identify overarching themes. The survey quantified sludge, delayed or forgone screenings, screening experience (Net Promoter Score) and health system distrust (Health System Distrust Scale). We used χ2 or t-tests for univariable comparisons and logistic or linear regressions to evaluate the association between cumulative sludge score and delayed or forgone screenings, screening experience and health system distrust. Results were integrated for interpretation.
Setting: Southeastern United States.
Participants: Patients who were 45-75 years of age, at average risk for CRC and had either completed or been referred for CRC screening (colonoscopy or stool-based test) within the previous 12 months.
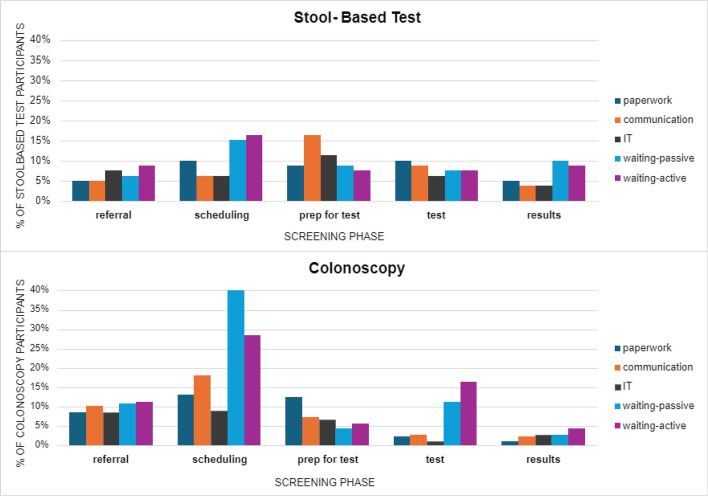
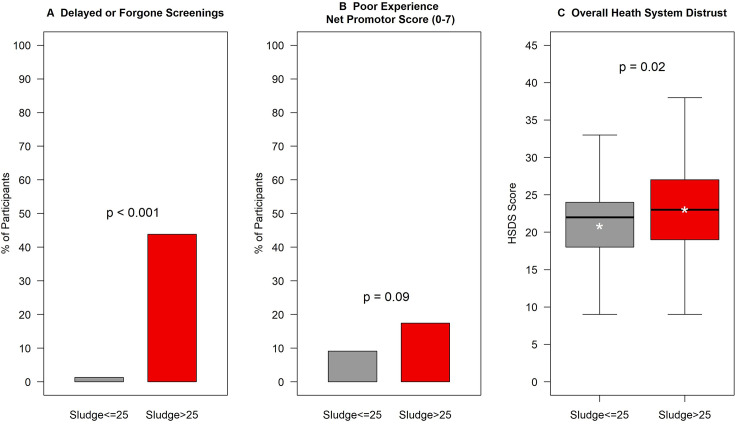
Results: 22 interview participants and 255 survey participants completed the study. 38 (15%) survey participants rated their screening experience as poor (Net Promoter Score=0-7 out of 10). The mean (SD) Health System Distrust Scale score was 22.4 (6.3) out of 45 possible points (higher score=greater distrust). Perceptions of sludge in the CRC screening process varied, with long waiting times and burdensome communication being the most common sources (58% and 35% of participants, respectively). Sludge was positively associated with delayed or forgone screenings (OR=1.42, 95% CI 1.28, 1.57, p<0.001), poor screening experience (OR=1.15, 95% CI 1.04, 1.28, p=0.009) and health system distrust (β=0.47, p<0.001). Qualitative findings add descriptive detail about sludge encountered, context to impacts experienced, and illustrate the heavy emotional impact of sludge: 'it just isn't worth it'.
Conclusion: Efforts to reduce sludge in the CRC screening process may improve timely completion of CRC screening, enhance patient experience and restore trust in the health system.
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
