Brian C. Westbrook , Laura J. Taylor , Eric Wallace , Marisa B. Marques , Jori E. May
{"title":"基于血小板计数的临床决策支持系统在帮助诊断肝素诱导的血小板减少症方面的局限性","authors":"Brian C. Westbrook , Laura J. Taylor , Eric Wallace , Marisa B. Marques , Jori E. May","doi":"10.1016/j.thromres.2024.109171","DOIUrl":null,"url":null,"abstract":"<div><div>Heparin-induced thrombocytopenia (HIT) is a rare complication of heparin exposure with potential for significant morbidity and mortality. Early identification and treatment can prevent catastrophic thrombosis. Herein, we report the performance of a platelet count-based clinical decision support system (CDSS) where providers received a notification when a patient had a platelet count decline of ≥50 %. In the 90-day study period, the CDSS sent 302 notifications on 270 patients. Notifications were frequently inappropriate; 25 % had an expected platelet count decline (organ donation, stem cell transplant), an inaccurate count, or no heparin exposure. Patient testing for HIT prompted by the CDSS was not in accordance with best practice guidelines in most circumstances. For example, 36 % had a low probability 4Ts score, while 42 % with an intermediate or high probability 4Ts score were not tested. Due to concern for lack of efficacy, the CDSS was discontinued. Analysis of an 8-month period before and after discontinuation showed a significant decrease in the number of enzyme immunoassays ordered (547 vs. 386) without a change in the number of patients with HIT identified (13 vs. 13) or the rate of thrombosis in those with confirmed HIT (62 % vs. 62 %). In conclusion, a CDSS based on platelet count decline contributed to “alert fatigue” via inappropriate notification and did not improve evidence-based HIT testing. In addition, its removal did not decrease or delay HIT identification. Additional efforts are needed to better define how CDSS can support the rapid diagnosis and appropriate treatment of patients with HIT.</div></div>","PeriodicalId":23064,"journal":{"name":"Thrombosis research","volume":"243 ","pages":"Article 109171"},"PeriodicalIF":3.4000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Limitations of a platelet count-based clinical decision support system to facilitate diagnosis of heparin-induced thrombocytopenia\",\"authors\":\"Brian C. Westbrook , Laura J. Taylor , Eric Wallace , Marisa B. Marques , Jori E. May\",\"doi\":\"10.1016/j.thromres.2024.109171\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><div>Heparin-induced thrombocytopenia (HIT) is a rare complication of heparin exposure with potential for significant morbidity and mortality. Early identification and treatment can prevent catastrophic thrombosis. Herein, we report the performance of a platelet count-based clinical decision support system (CDSS) where providers received a notification when a patient had a platelet count decline of ≥50 %. In the 90-day study period, the CDSS sent 302 notifications on 270 patients. Notifications were frequently inappropriate; 25 % had an expected platelet count decline (organ donation, stem cell transplant), an inaccurate count, or no heparin exposure. Patient testing for HIT prompted by the CDSS was not in accordance with best practice guidelines in most circumstances. For example, 36 % had a low probability 4Ts score, while 42 % with an intermediate or high probability 4Ts score were not tested. Due to concern for lack of efficacy, the CDSS was discontinued. Analysis of an 8-month period before and after discontinuation showed a significant decrease in the number of enzyme immunoassays ordered (547 vs. 386) without a change in the number of patients with HIT identified (13 vs. 13) or the rate of thrombosis in those with confirmed HIT (62 % vs. 62 %). In conclusion, a CDSS based on platelet count decline contributed to “alert fatigue” via inappropriate notification and did not improve evidence-based HIT testing. In addition, its removal did not decrease or delay HIT identification. Additional efforts are needed to better define how CDSS can support the rapid diagnosis and appropriate treatment of patients with HIT.</div></div>\",\"PeriodicalId\":23064,\"journal\":{\"name\":\"Thrombosis research\",\"volume\":\"243 \",\"pages\":\"Article 109171\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thrombosis research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0049384824003037\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thrombosis research","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0049384824003037","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
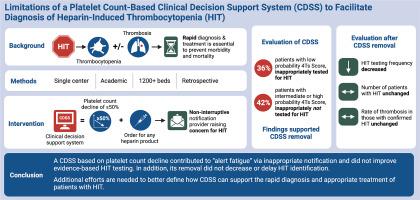
肝素诱导的血小板减少症(HIT)是一种罕见的肝素暴露并发症,可能导致严重的发病率和死亡率。早期识别和治疗可以预防灾难性血栓形成。在本文中,我们报告了基于血小板计数的临床决策支持系统(CDSS)的性能,当患者血小板计数下降≥50%时,医疗服务提供者会收到通知。在 90 天的研究期间,CDSS 向 270 名患者发送了 302 次通知。通知往往不恰当;25%的患者血小板计数下降在意料之中(器官捐献、干细胞移植)、计数不准确或未接触肝素。在大多数情况下,CDSS 提示患者进行 HIT 检测并不符合最佳实践指南。例如,有 36% 的患者的 4Ts 评分为低概率,而 42% 的患者的 4Ts 评分为中概率或高概率,却没有进行检测。由于担心缺乏疗效,CDSS 停止使用。对停用前后 8 个月的分析表明,订购酶免疫测定的数量显著减少(547 对 386),但确定的 HIT 患者人数(13 对 13)或确诊 HIT 患者的血栓形成率(62% 对 62%)均无变化。总之,基于血小板计数下降的 CDSS 通过不适当的通知造成了 "警报疲劳",并没有改善循证 HIT 检测。此外,取消 CDSS 并没有减少或延迟 HIT 识别。还需要进一步努力,以更好地确定 CDSS 如何支持 HIT 患者的快速诊断和适当治疗。
Limitations of a platelet count-based clinical decision support system to facilitate diagnosis of heparin-induced thrombocytopenia
Heparin-induced thrombocytopenia (HIT) is a rare complication of heparin exposure with potential for significant morbidity and mortality. Early identification and treatment can prevent catastrophic thrombosis. Herein, we report the performance of a platelet count-based clinical decision support system (CDSS) where providers received a notification when a patient had a platelet count decline of ≥50 %. In the 90-day study period, the CDSS sent 302 notifications on 270 patients. Notifications were frequently inappropriate; 25 % had an expected platelet count decline (organ donation, stem cell transplant), an inaccurate count, or no heparin exposure. Patient testing for HIT prompted by the CDSS was not in accordance with best practice guidelines in most circumstances. For example, 36 % had a low probability 4Ts score, while 42 % with an intermediate or high probability 4Ts score were not tested. Due to concern for lack of efficacy, the CDSS was discontinued. Analysis of an 8-month period before and after discontinuation showed a significant decrease in the number of enzyme immunoassays ordered (547 vs. 386) without a change in the number of patients with HIT identified (13 vs. 13) or the rate of thrombosis in those with confirmed HIT (62 % vs. 62 %). In conclusion, a CDSS based on platelet count decline contributed to “alert fatigue” via inappropriate notification and did not improve evidence-based HIT testing. In addition, its removal did not decrease or delay HIT identification. Additional efforts are needed to better define how CDSS can support the rapid diagnosis and appropriate treatment of patients with HIT.
期刊介绍:
Thrombosis Research is an international journal dedicated to the swift dissemination of new information on thrombosis, hemostasis, and vascular biology, aimed at advancing both science and clinical care. The journal publishes peer-reviewed original research, reviews, editorials, opinions, and critiques, covering both basic and clinical studies. Priority is given to research that promises novel approaches in the diagnosis, therapy, prognosis, and prevention of thrombotic and hemorrhagic diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
