{"title":"家庭照护者的生活经验对家庭和社区服务至关重要。","authors":"Nathan A. Boucher DrPH, PA, MS, MPA, CPHQ","doi":"10.1111/jgs.19120","DOIUrl":null,"url":null,"abstract":"<p>In this issue of the Journal, Trivedi et al. (<i>not sure about final citation</i>) use in-depth interviews with family caregivers of Veterans to identify novel intervention targets to help the field improve awareness, access, and use of home- and community-based services (HCBS) among family caregivers. The authors now help me make a clarion call for the importance of engaging family caregivers—those family (sometimes friends/neighbors) bearing the joys and burdens of community-based care and support. Optimal support for aging adults and those living with disabilities in our community pivots on the awareness, willingness, skills, and time of family caregivers.</p><p>Inquiries such as this from Trivedi et al. are both timely and important. Their work reflects adherence to tenets of person-centeredness and community engagement trumpeted by recent reports such as the U.S. Department of Health and Human Services' Interagency Coordinating Committee on Healthy Aging and Age-Friendly Communities in May 2024, which explicitly calls out the role of family caregivers in community-based care.<span><sup>1</sup></span> The voices of family caregivers in the provision of HCBS need to be amplified as US health care and payment for that care are rebalanced toward community-based solutions and away from facility-based care.<span><sup>2</sup></span></p><p>The authors studied a critical context: family caregivers supporting Veterans served by the largest comprehensive healthcare system in the United States, the Veterans Administration (VA). Importantly, the VA pushes innovations in health systems research attuned to aging, disability, and caregiver inclusion,<span><sup>3-6</sup></span> but, as Trivedi et al. note, HCBS continue to be underutilized by Veterans and others. Complicating this, HCBS are under-resourced in many areas including direct care workers<span><sup>7</sup></span> who often work in tandem with family caregivers cobbling together ongoing services for the aging and those living with disabilities.<span><sup>1</sup></span> Well-supported family caregivers are crucial to the intended expansion in HCBS across populations.<span><sup>8, 9</sup></span></p><p>The authors bring to the readers of the Journal insights on barriers to optimal use of HCBS. They accomplish this by focusing not just on logistical issues—challenges known and persistent—but, more uniquely, psychosocial and interpersonal barriers to accessing VA and non-VA HCBS alike using two complementary research methods.</p><p>First, the authors conducted semi-structured interviews with caregivers. This was elegantly guided by Andersen's Behavioral Model of Health Services Use.<span><sup>10</sup></span> The first three resulting themes are not necessarily new but help bolster findings in the Veteran caregiver population where fewer studies reside. The authors found that caregivers experience gaps in accurate and timely information from the VA and community organizations; they lack time and experience opportunity costs; and they desire respite, which allows them to take breaks from the work of caregiving and to take time for themselves. Health system leaders have clear areas on which to focus system improvements, articulated effectively by Trivedi et al. The fourth theme—strain on the interpersonal relationship further inhibiting the use of HCBS—is a novel finding and very much resonates with me after some years working with Veterans and their families. Personal pride and self-reliance play roles in Veterans lives<span><sup>11</sup></span> and certainly in the lives of those with whom I have connected in the Veteran community. What happens when pride manifests as refusal to seek help and, in the case of the authors' findings, creates a rift in the way care recipient and caregiver make decisions together? This barrier is not small and may reduce engagement with needed services and supports. Always leading with validation of their accomplishments to date seems to be the better way to engage with this population in my experience. Additionally, tapping into the idea of teamwork, so ingrained in military culture, is another useful strategy—acknowledging we all need help across the great expanse of life.</p><p>Second, embedded in the interview, the author team had participants complete a checklist of services and supports typically falling under HCBS. Importantly, participants could indicate not knowing about the service or support, knowing about it and not using it, or using it now or in the past. While not validated, the measure is clear and useful in my view and dovetails well with the qualitative interviews. Lack of awareness of VA caregiver support services and other community-based services is evident in this sample mirroring our own findings in a sample of caregivers and Veterans in the context of serious illness.<span><sup>12</sup></span> Even when aware of available services/supports, the pandemic hobbled caregivers' access to these services/supports in Trivedi et al.'s study. Caregivers should be supported by systems of care to overcome temporary events whether they are relatively rare like a pandemic or frequent like hurricanes—either poses challenges for caregiving by curtailing access to services and supports.<span><sup>13</sup></span></p><p>There are some limitations, as the authors note, such as the setting being urban/suburban and relatively affluent. Therefore, some challenges experienced by family caregivers in less affluent and more rural areas may be missing. This helps highlight the need, in my view, for a refocus of our research efforts on reaching participants beyond the vicinity of our academic centers to more rural and less affluent areas. If it takes you more effort to reach them, you may be innovating in real time, and this will help push our research forward. With our collective research prowess, we can recruit creatively and shrink distances. In recent work, we came to realize the reliable telephone must remain a participant's option when lack of costly computer hardware or limited rural internet bandwidth pose barriers, to say nothing of additional challenges imposed by arranging in-person research engagements. In the case of Trivedi et al.'s study, a pandemic also made telephone a safe and sensible option.</p><p>Recruitment was a challenge during the coronavirus pandemic but, I would argue, a perennial challenge in caregiving research. Caregivers are busy people, and this is readily illustrated by Trivedi et al.—caregivers expressed having little time to care for their Veteran or themselves. Capturing caregivers' time takes a researcher's patience, ingenuity, and empathy. Researchers would do well to offer compensation, flexibility in scheduling/rescheduling, communication choices (e.g., web-based, telephone, in-person), and the opportunity for caregivers to continue some caregiving during data collection. This latter approach may, for example, call on study staff to lend a hand at a research site when a care recipient arrives with a caregiver research participant or assist in sanctioned and reasonable ways when collecting data in the home. Thoughtful attention to revising research protocols for these types of engagements is in order.</p><p>My vision for the future aligns well with Trivedi and colleagues: placing caregivers in the conversation and learning from their experiences—after all, who knows their care recipient best? Yes, there is less availability of some resources in rural communities, for example, but we hear from caregivers frequently that they know there are services available, but they do not have the time to research them and connect themselves. Reducing this time burden, effectively reducing caregiver stress, could be assisted by navigator and community health worker (CHW)-type programs focused on bridging the gap between systems of care and support and proactively connecting caregivers to solve their identified needs.<span><sup>14-16</sup></span> This additional layer of human support could work as an adjunct to what the VA already does to support caregivers, which is substantial compared with non-VA systems of care.<span><sup>17</sup></span> Figure 1 simply shows a CHW supporting a caregiver and connecting them to existing services within the VA and in their community. I characterize this connection in the following steps: (1) CHWs assess the needs of caregivers and problem solve with them to find solutions. (2) CHWs facilitate linkages to services liberating caregivers to focus on direct care of Veterans. (3) CHWs offer weekly check-ins and are available as needed to listen to caregivers' concerns and strategize approaches. (4) Caregivers have the CHW as a point of contact for strategizing how to obtain VA and community services/supports. (5) Successful connection to services would reduce caregiver burden by meeting unmet needs and allowing more caregiver capacity for self-care and caregiving.</p><p>In conclusion, it is my hope that this Journal's readership—influential clinicians and leaders across diverse health systems—read Trivedi et al. with care. May readers be reminded or now fully realize that improving access to HCBS not only necessitates macro-level interventions addressing systems-level barriers but also micro-level interventions mitigating stress for family caregivers and those for whom they care each day.</p><p>Dr. Boucher was the sole contributor to this manuscript.</p><p>The author declares no conflicts of interest.</p><p>The author declares no role for any sponsor in the preparation of this manuscript.</p><p>The author declares no financial disclosures. The opinion expressed is that of the author and does not reflect those of Duke University, Department of Veterans Affairs, or the U.S. Government.</p>","PeriodicalId":17240,"journal":{"name":"Journal of the American Geriatrics Society","volume":"72 11","pages":"3296-3298"},"PeriodicalIF":4.3000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19120","citationCount":"0","resultStr":"{\"title\":\"Family caregiver lived experience matters in home- and community-based services\",\"authors\":\"Nathan A. Boucher DrPH, PA, MS, MPA, CPHQ\",\"doi\":\"10.1111/jgs.19120\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In this issue of the Journal, Trivedi et al. (<i>not sure about final citation</i>) use in-depth interviews with family caregivers of Veterans to identify novel intervention targets to help the field improve awareness, access, and use of home- and community-based services (HCBS) among family caregivers. The authors now help me make a clarion call for the importance of engaging family caregivers—those family (sometimes friends/neighbors) bearing the joys and burdens of community-based care and support. Optimal support for aging adults and those living with disabilities in our community pivots on the awareness, willingness, skills, and time of family caregivers.</p><p>Inquiries such as this from Trivedi et al. are both timely and important. Their work reflects adherence to tenets of person-centeredness and community engagement trumpeted by recent reports such as the U.S. Department of Health and Human Services' Interagency Coordinating Committee on Healthy Aging and Age-Friendly Communities in May 2024, which explicitly calls out the role of family caregivers in community-based care.<span><sup>1</sup></span> The voices of family caregivers in the provision of HCBS need to be amplified as US health care and payment for that care are rebalanced toward community-based solutions and away from facility-based care.<span><sup>2</sup></span></p><p>The authors studied a critical context: family caregivers supporting Veterans served by the largest comprehensive healthcare system in the United States, the Veterans Administration (VA). Importantly, the VA pushes innovations in health systems research attuned to aging, disability, and caregiver inclusion,<span><sup>3-6</sup></span> but, as Trivedi et al. note, HCBS continue to be underutilized by Veterans and others. Complicating this, HCBS are under-resourced in many areas including direct care workers<span><sup>7</sup></span> who often work in tandem with family caregivers cobbling together ongoing services for the aging and those living with disabilities.<span><sup>1</sup></span> Well-supported family caregivers are crucial to the intended expansion in HCBS across populations.<span><sup>8, 9</sup></span></p><p>The authors bring to the readers of the Journal insights on barriers to optimal use of HCBS. They accomplish this by focusing not just on logistical issues—challenges known and persistent—but, more uniquely, psychosocial and interpersonal barriers to accessing VA and non-VA HCBS alike using two complementary research methods.</p><p>First, the authors conducted semi-structured interviews with caregivers. This was elegantly guided by Andersen's Behavioral Model of Health Services Use.<span><sup>10</sup></span> The first three resulting themes are not necessarily new but help bolster findings in the Veteran caregiver population where fewer studies reside. The authors found that caregivers experience gaps in accurate and timely information from the VA and community organizations; they lack time and experience opportunity costs; and they desire respite, which allows them to take breaks from the work of caregiving and to take time for themselves. Health system leaders have clear areas on which to focus system improvements, articulated effectively by Trivedi et al. The fourth theme—strain on the interpersonal relationship further inhibiting the use of HCBS—is a novel finding and very much resonates with me after some years working with Veterans and their families. Personal pride and self-reliance play roles in Veterans lives<span><sup>11</sup></span> and certainly in the lives of those with whom I have connected in the Veteran community. What happens when pride manifests as refusal to seek help and, in the case of the authors' findings, creates a rift in the way care recipient and caregiver make decisions together? This barrier is not small and may reduce engagement with needed services and supports. Always leading with validation of their accomplishments to date seems to be the better way to engage with this population in my experience. Additionally, tapping into the idea of teamwork, so ingrained in military culture, is another useful strategy—acknowledging we all need help across the great expanse of life.</p><p>Second, embedded in the interview, the author team had participants complete a checklist of services and supports typically falling under HCBS. Importantly, participants could indicate not knowing about the service or support, knowing about it and not using it, or using it now or in the past. While not validated, the measure is clear and useful in my view and dovetails well with the qualitative interviews. Lack of awareness of VA caregiver support services and other community-based services is evident in this sample mirroring our own findings in a sample of caregivers and Veterans in the context of serious illness.<span><sup>12</sup></span> Even when aware of available services/supports, the pandemic hobbled caregivers' access to these services/supports in Trivedi et al.'s study. Caregivers should be supported by systems of care to overcome temporary events whether they are relatively rare like a pandemic or frequent like hurricanes—either poses challenges for caregiving by curtailing access to services and supports.<span><sup>13</sup></span></p><p>There are some limitations, as the authors note, such as the setting being urban/suburban and relatively affluent. Therefore, some challenges experienced by family caregivers in less affluent and more rural areas may be missing. This helps highlight the need, in my view, for a refocus of our research efforts on reaching participants beyond the vicinity of our academic centers to more rural and less affluent areas. If it takes you more effort to reach them, you may be innovating in real time, and this will help push our research forward. With our collective research prowess, we can recruit creatively and shrink distances. In recent work, we came to realize the reliable telephone must remain a participant's option when lack of costly computer hardware or limited rural internet bandwidth pose barriers, to say nothing of additional challenges imposed by arranging in-person research engagements. In the case of Trivedi et al.'s study, a pandemic also made telephone a safe and sensible option.</p><p>Recruitment was a challenge during the coronavirus pandemic but, I would argue, a perennial challenge in caregiving research. Caregivers are busy people, and this is readily illustrated by Trivedi et al.—caregivers expressed having little time to care for their Veteran or themselves. Capturing caregivers' time takes a researcher's patience, ingenuity, and empathy. Researchers would do well to offer compensation, flexibility in scheduling/rescheduling, communication choices (e.g., web-based, telephone, in-person), and the opportunity for caregivers to continue some caregiving during data collection. This latter approach may, for example, call on study staff to lend a hand at a research site when a care recipient arrives with a caregiver research participant or assist in sanctioned and reasonable ways when collecting data in the home. Thoughtful attention to revising research protocols for these types of engagements is in order.</p><p>My vision for the future aligns well with Trivedi and colleagues: placing caregivers in the conversation and learning from their experiences—after all, who knows their care recipient best? Yes, there is less availability of some resources in rural communities, for example, but we hear from caregivers frequently that they know there are services available, but they do not have the time to research them and connect themselves. Reducing this time burden, effectively reducing caregiver stress, could be assisted by navigator and community health worker (CHW)-type programs focused on bridging the gap between systems of care and support and proactively connecting caregivers to solve their identified needs.<span><sup>14-16</sup></span> This additional layer of human support could work as an adjunct to what the VA already does to support caregivers, which is substantial compared with non-VA systems of care.<span><sup>17</sup></span> Figure 1 simply shows a CHW supporting a caregiver and connecting them to existing services within the VA and in their community. I characterize this connection in the following steps: (1) CHWs assess the needs of caregivers and problem solve with them to find solutions. (2) CHWs facilitate linkages to services liberating caregivers to focus on direct care of Veterans. (3) CHWs offer weekly check-ins and are available as needed to listen to caregivers' concerns and strategize approaches. (4) Caregivers have the CHW as a point of contact for strategizing how to obtain VA and community services/supports. (5) Successful connection to services would reduce caregiver burden by meeting unmet needs and allowing more caregiver capacity for self-care and caregiving.</p><p>In conclusion, it is my hope that this Journal's readership—influential clinicians and leaders across diverse health systems—read Trivedi et al. with care. May readers be reminded or now fully realize that improving access to HCBS not only necessitates macro-level interventions addressing systems-level barriers but also micro-level interventions mitigating stress for family caregivers and those for whom they care each day.</p><p>Dr. Boucher was the sole contributor to this manuscript.</p><p>The author declares no conflicts of interest.</p><p>The author declares no role for any sponsor in the preparation of this manuscript.</p><p>The author declares no financial disclosures. The opinion expressed is that of the author and does not reflect those of Duke University, Department of Veterans Affairs, or the U.S. Government.</p>\",\"PeriodicalId\":17240,\"journal\":{\"name\":\"Journal of the American Geriatrics Society\",\"volume\":\"72 11\",\"pages\":\"3296-3298\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.19120\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the American Geriatrics Society\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19120\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Geriatrics Society","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgs.19120","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Family caregiver lived experience matters in home- and community-based services
In this issue of the Journal, Trivedi et al. (not sure about final citation) use in-depth interviews with family caregivers of Veterans to identify novel intervention targets to help the field improve awareness, access, and use of home- and community-based services (HCBS) among family caregivers. The authors now help me make a clarion call for the importance of engaging family caregivers—those family (sometimes friends/neighbors) bearing the joys and burdens of community-based care and support. Optimal support for aging adults and those living with disabilities in our community pivots on the awareness, willingness, skills, and time of family caregivers.
Inquiries such as this from Trivedi et al. are both timely and important. Their work reflects adherence to tenets of person-centeredness and community engagement trumpeted by recent reports such as the U.S. Department of Health and Human Services' Interagency Coordinating Committee on Healthy Aging and Age-Friendly Communities in May 2024, which explicitly calls out the role of family caregivers in community-based care.1 The voices of family caregivers in the provision of HCBS need to be amplified as US health care and payment for that care are rebalanced toward community-based solutions and away from facility-based care.2
The authors studied a critical context: family caregivers supporting Veterans served by the largest comprehensive healthcare system in the United States, the Veterans Administration (VA). Importantly, the VA pushes innovations in health systems research attuned to aging, disability, and caregiver inclusion,3-6 but, as Trivedi et al. note, HCBS continue to be underutilized by Veterans and others. Complicating this, HCBS are under-resourced in many areas including direct care workers7 who often work in tandem with family caregivers cobbling together ongoing services for the aging and those living with disabilities.1 Well-supported family caregivers are crucial to the intended expansion in HCBS across populations.8, 9
The authors bring to the readers of the Journal insights on barriers to optimal use of HCBS. They accomplish this by focusing not just on logistical issues—challenges known and persistent—but, more uniquely, psychosocial and interpersonal barriers to accessing VA and non-VA HCBS alike using two complementary research methods.
First, the authors conducted semi-structured interviews with caregivers. This was elegantly guided by Andersen's Behavioral Model of Health Services Use.10 The first three resulting themes are not necessarily new but help bolster findings in the Veteran caregiver population where fewer studies reside. The authors found that caregivers experience gaps in accurate and timely information from the VA and community organizations; they lack time and experience opportunity costs; and they desire respite, which allows them to take breaks from the work of caregiving and to take time for themselves. Health system leaders have clear areas on which to focus system improvements, articulated effectively by Trivedi et al. The fourth theme—strain on the interpersonal relationship further inhibiting the use of HCBS—is a novel finding and very much resonates with me after some years working with Veterans and their families. Personal pride and self-reliance play roles in Veterans lives11 and certainly in the lives of those with whom I have connected in the Veteran community. What happens when pride manifests as refusal to seek help and, in the case of the authors' findings, creates a rift in the way care recipient and caregiver make decisions together? This barrier is not small and may reduce engagement with needed services and supports. Always leading with validation of their accomplishments to date seems to be the better way to engage with this population in my experience. Additionally, tapping into the idea of teamwork, so ingrained in military culture, is another useful strategy—acknowledging we all need help across the great expanse of life.
Second, embedded in the interview, the author team had participants complete a checklist of services and supports typically falling under HCBS. Importantly, participants could indicate not knowing about the service or support, knowing about it and not using it, or using it now or in the past. While not validated, the measure is clear and useful in my view and dovetails well with the qualitative interviews. Lack of awareness of VA caregiver support services and other community-based services is evident in this sample mirroring our own findings in a sample of caregivers and Veterans in the context of serious illness.12 Even when aware of available services/supports, the pandemic hobbled caregivers' access to these services/supports in Trivedi et al.'s study. Caregivers should be supported by systems of care to overcome temporary events whether they are relatively rare like a pandemic or frequent like hurricanes—either poses challenges for caregiving by curtailing access to services and supports.13
There are some limitations, as the authors note, such as the setting being urban/suburban and relatively affluent. Therefore, some challenges experienced by family caregivers in less affluent and more rural areas may be missing. This helps highlight the need, in my view, for a refocus of our research efforts on reaching participants beyond the vicinity of our academic centers to more rural and less affluent areas. If it takes you more effort to reach them, you may be innovating in real time, and this will help push our research forward. With our collective research prowess, we can recruit creatively and shrink distances. In recent work, we came to realize the reliable telephone must remain a participant's option when lack of costly computer hardware or limited rural internet bandwidth pose barriers, to say nothing of additional challenges imposed by arranging in-person research engagements. In the case of Trivedi et al.'s study, a pandemic also made telephone a safe and sensible option.
Recruitment was a challenge during the coronavirus pandemic but, I would argue, a perennial challenge in caregiving research. Caregivers are busy people, and this is readily illustrated by Trivedi et al.—caregivers expressed having little time to care for their Veteran or themselves. Capturing caregivers' time takes a researcher's patience, ingenuity, and empathy. Researchers would do well to offer compensation, flexibility in scheduling/rescheduling, communication choices (e.g., web-based, telephone, in-person), and the opportunity for caregivers to continue some caregiving during data collection. This latter approach may, for example, call on study staff to lend a hand at a research site when a care recipient arrives with a caregiver research participant or assist in sanctioned and reasonable ways when collecting data in the home. Thoughtful attention to revising research protocols for these types of engagements is in order.
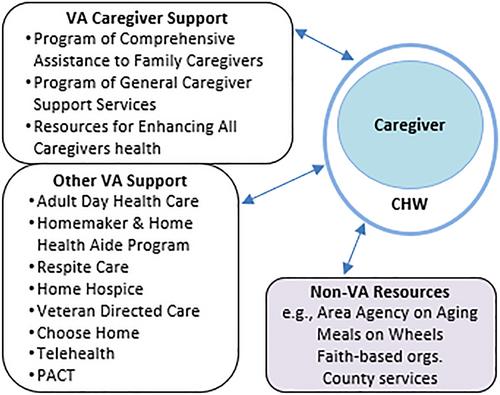
My vision for the future aligns well with Trivedi and colleagues: placing caregivers in the conversation and learning from their experiences—after all, who knows their care recipient best? Yes, there is less availability of some resources in rural communities, for example, but we hear from caregivers frequently that they know there are services available, but they do not have the time to research them and connect themselves. Reducing this time burden, effectively reducing caregiver stress, could be assisted by navigator and community health worker (CHW)-type programs focused on bridging the gap between systems of care and support and proactively connecting caregivers to solve their identified needs.14-16 This additional layer of human support could work as an adjunct to what the VA already does to support caregivers, which is substantial compared with non-VA systems of care.17 Figure 1 simply shows a CHW supporting a caregiver and connecting them to existing services within the VA and in their community. I characterize this connection in the following steps: (1) CHWs assess the needs of caregivers and problem solve with them to find solutions. (2) CHWs facilitate linkages to services liberating caregivers to focus on direct care of Veterans. (3) CHWs offer weekly check-ins and are available as needed to listen to caregivers' concerns and strategize approaches. (4) Caregivers have the CHW as a point of contact for strategizing how to obtain VA and community services/supports. (5) Successful connection to services would reduce caregiver burden by meeting unmet needs and allowing more caregiver capacity for self-care and caregiving.
In conclusion, it is my hope that this Journal's readership—influential clinicians and leaders across diverse health systems—read Trivedi et al. with care. May readers be reminded or now fully realize that improving access to HCBS not only necessitates macro-level interventions addressing systems-level barriers but also micro-level interventions mitigating stress for family caregivers and those for whom they care each day.
Dr. Boucher was the sole contributor to this manuscript.
The author declares no conflicts of interest.
The author declares no role for any sponsor in the preparation of this manuscript.
The author declares no financial disclosures. The opinion expressed is that of the author and does not reflect those of Duke University, Department of Veterans Affairs, or the U.S. Government.
期刊介绍:
Journal of the American Geriatrics Society (JAGS) is the go-to journal for clinical aging research. We provide a diverse, interprofessional community of healthcare professionals with the latest insights on geriatrics education, clinical practice, and public policy—all supporting the high-quality, person-centered care essential to our well-being as we age. Since the publication of our first edition in 1953, JAGS has remained one of the oldest and most impactful journals dedicated exclusively to gerontology and geriatrics.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
