{"title":"评估神经性厌食症患者的肾功能。","authors":"Hiroyuki Miyahara, Yoshie Shigeyasu, Chikako Fujii, Chie Tanaka, Mana Hanzawa, Akiko Sugihara, Ayumi Okada, Hirokazu Tsukahara","doi":"10.1186/s13030-024-00316-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A decreased glomerular filtration rate (GFR), estimated using creatinine (Cr- eGFR), is often found at the initial presentation of anorexia nervosa (AN). Its pathophysiology has been explained mainly by dehydration, and chronic hypokalemia is also thought to be a cause. However, because we have often experienced cases of AN with decreased Cr-eGFR without these conditions, we must consider different etiologies. The focus of this paper is on low free triiodothyronine (FT3) syndrome. We also discuss the utility of eGFR, estimated using cystatin-C (CysC-eGFR), for these patients.</p><p><strong>Methods: </strong>The data of 39 patients diagnosed with AN between January 2005 and December 2023 was available for study. The characteristics of patients at the lowest and highest body mass index standard deviation score (BMI-SDS) were examined. Data on the parameters Cr-eGFR, CysC-eGFR, dehydration markers, potassium (K), and hormonal data and BMI-SDS were assessed during the treatment course to evaluate the correlations in these parameters. Blood hematocrit, uric acid (UA), blood urine nitrogen (BUN) level, and urine specific gravity were adopted as dehydration markers; FT3, free thyroxine, thyroid stimulating hormone, and insulin-like growth factor were adopted as hormonal data. Cr-eGFR and simultaneously evaluated dehydration markers, K, or hormonal data were extracted and correlations associated with the changes in BMI-SDS were examined. Furthermore, Cr-eGFR and simultaneously assessed CysC-eGFR were compared.</p><p><strong>Results: </strong>When the BMI-SDS was at the lowest value, low-FT3 syndrome was shown. Severe hypokalemia was not found in our study. A linear relation was not found between Cr-eGFR and BMI-SDS. A statistically significant correlation was found between Cr-eGFR and FT3 (p = 0.0025). Among the dehydration markers, statistically significant correlations were found between Cr-eGFR and BUN or UA. The difference between Cr-eGFR and CysC-eGFR was prominent, and CysC-eGFR showed much higher values.</p><p><strong>Conclusions: </strong>Our data indicates that low-FT3 syndrome and dehydration were related to the renal function of our patients with AN. Furthermore, our data suggest that caution is needed in the interpretation of kidney function evaluation when using CysC-eGFR in cases of AN.</p>","PeriodicalId":9027,"journal":{"name":"BioPsychoSocial Medicine","volume":"18 1","pages":"19"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11439319/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessment of the renal function of patients with anorexia nervosa.\",\"authors\":\"Hiroyuki Miyahara, Yoshie Shigeyasu, Chikako Fujii, Chie Tanaka, Mana Hanzawa, Akiko Sugihara, Ayumi Okada, Hirokazu Tsukahara\",\"doi\":\"10.1186/s13030-024-00316-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A decreased glomerular filtration rate (GFR), estimated using creatinine (Cr- eGFR), is often found at the initial presentation of anorexia nervosa (AN). Its pathophysiology has been explained mainly by dehydration, and chronic hypokalemia is also thought to be a cause. However, because we have often experienced cases of AN with decreased Cr-eGFR without these conditions, we must consider different etiologies. The focus of this paper is on low free triiodothyronine (FT3) syndrome. We also discuss the utility of eGFR, estimated using cystatin-C (CysC-eGFR), for these patients.</p><p><strong>Methods: </strong>The data of 39 patients diagnosed with AN between January 2005 and December 2023 was available for study. The characteristics of patients at the lowest and highest body mass index standard deviation score (BMI-SDS) were examined. Data on the parameters Cr-eGFR, CysC-eGFR, dehydration markers, potassium (K), and hormonal data and BMI-SDS were assessed during the treatment course to evaluate the correlations in these parameters. Blood hematocrit, uric acid (UA), blood urine nitrogen (BUN) level, and urine specific gravity were adopted as dehydration markers; FT3, free thyroxine, thyroid stimulating hormone, and insulin-like growth factor were adopted as hormonal data. Cr-eGFR and simultaneously evaluated dehydration markers, K, or hormonal data were extracted and correlations associated with the changes in BMI-SDS were examined. Furthermore, Cr-eGFR and simultaneously assessed CysC-eGFR were compared.</p><p><strong>Results: </strong>When the BMI-SDS was at the lowest value, low-FT3 syndrome was shown. Severe hypokalemia was not found in our study. A linear relation was not found between Cr-eGFR and BMI-SDS. A statistically significant correlation was found between Cr-eGFR and FT3 (p = 0.0025). Among the dehydration markers, statistically significant correlations were found between Cr-eGFR and BUN or UA. The difference between Cr-eGFR and CysC-eGFR was prominent, and CysC-eGFR showed much higher values.</p><p><strong>Conclusions: </strong>Our data indicates that low-FT3 syndrome and dehydration were related to the renal function of our patients with AN. Furthermore, our data suggest that caution is needed in the interpretation of kidney function evaluation when using CysC-eGFR in cases of AN.</p>\",\"PeriodicalId\":9027,\"journal\":{\"name\":\"BioPsychoSocial Medicine\",\"volume\":\"18 1\",\"pages\":\"19\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-09-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11439319/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BioPsychoSocial Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13030-024-00316-6\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BioPsychoSocial Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13030-024-00316-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
摘要
背景:在神经性厌食症(AN)的初期症状中,通常会发现肾小球滤过率(GFR)下降,而肾小球滤过率是用肌酐(Cr- eGFR)来估算的。其病理生理学原因主要是脱水,慢性低钾血症也被认为是原因之一。然而,由于我们经常遇到的神经性厌食症患者在没有上述症状的情况下出现 Cr-eGFR 降低,因此我们必须考虑不同的病因。本文的重点是低游离三碘甲状腺原氨酸(FT3)综合征。我们还讨论了使用胱抑素-C(CysC-eGFR)估算的 eGFR 对这些患者的实用性:研究收集了 2005 年 1 月至 2023 年 12 月期间确诊的 39 例 AN 患者的数据。研究考察了体重指数标准差(BMI-SDS)最低和最高的患者的特征。在治疗过程中评估了Cr-eGFR、CysC-eGFR、脱水指标、钾(K)、激素数据和BMI-SDS等参数,以评估这些参数之间的相关性。脱水指标包括血细胞比容、尿酸(UA)、血尿氮(BUN)水平和尿比重;激素数据包括绒毛膜促性腺激素(FT3)、游离甲状腺素、促甲状腺激素和胰岛素样生长因子。提取 Cr-eGFR 和同时评估的脱水指标、K 或激素数据,并研究其与 BMI-SDS 变化的相关性。此外,还对 Cr-eGFR 和同时评估的 CysC-eGFR 进行了比较:结果:当 BMI-SDS 处于最低值时,出现低 FT3 综合征。我们的研究未发现严重的低钾血症。Cr-eGFR 与 BMI-SDS 之间未发现线性关系。Cr-eGFR 与 FT3 之间存在统计学意义上的相关性(p = 0.0025)。在脱水指标中,Cr-eGFR 与 BUN 或 UA 之间存在统计学意义上的显著相关性。Cr-eGFR与CysC-eGFR之间的差异非常明显,CysC-eGFR显示出更高的值:我们的数据表明,低 FT3 综合征和脱水与 AN 患者的肾功能有关。结论:我们的数据表明,低 FT3 综合征和脱水与 AN 患者的肾功能有关。此外,我们的数据还表明,在 AN 患者中使用 CysC-eGFR 进行肾功能评估时需要谨慎。
Assessment of the renal function of patients with anorexia nervosa.
Background: A decreased glomerular filtration rate (GFR), estimated using creatinine (Cr- eGFR), is often found at the initial presentation of anorexia nervosa (AN). Its pathophysiology has been explained mainly by dehydration, and chronic hypokalemia is also thought to be a cause. However, because we have often experienced cases of AN with decreased Cr-eGFR without these conditions, we must consider different etiologies. The focus of this paper is on low free triiodothyronine (FT3) syndrome. We also discuss the utility of eGFR, estimated using cystatin-C (CysC-eGFR), for these patients.
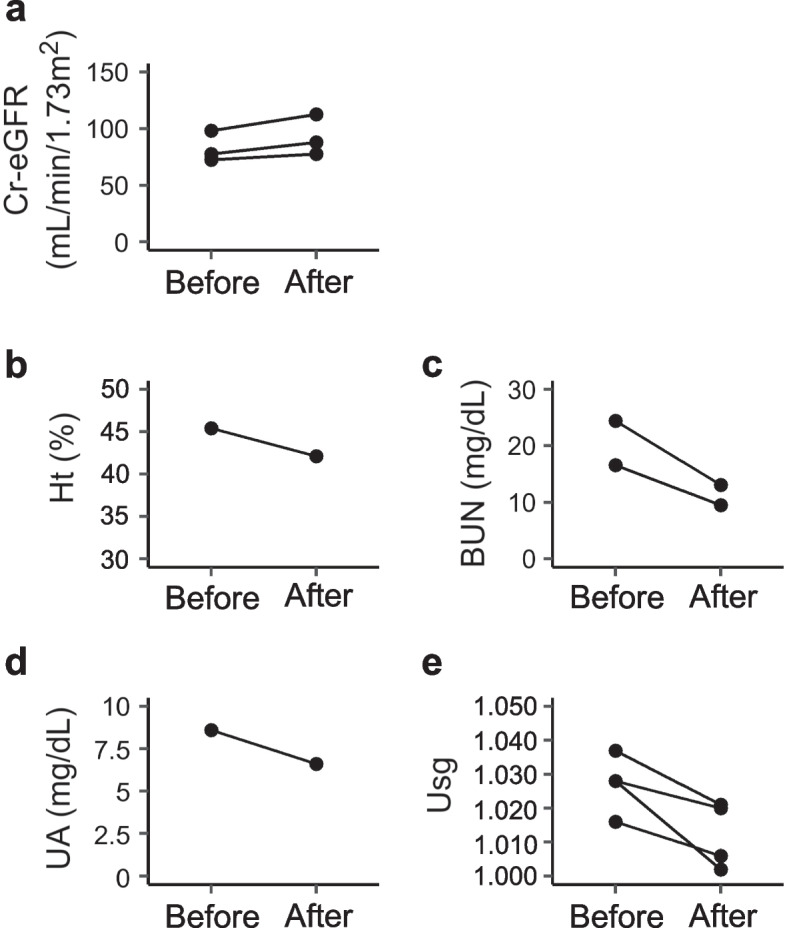
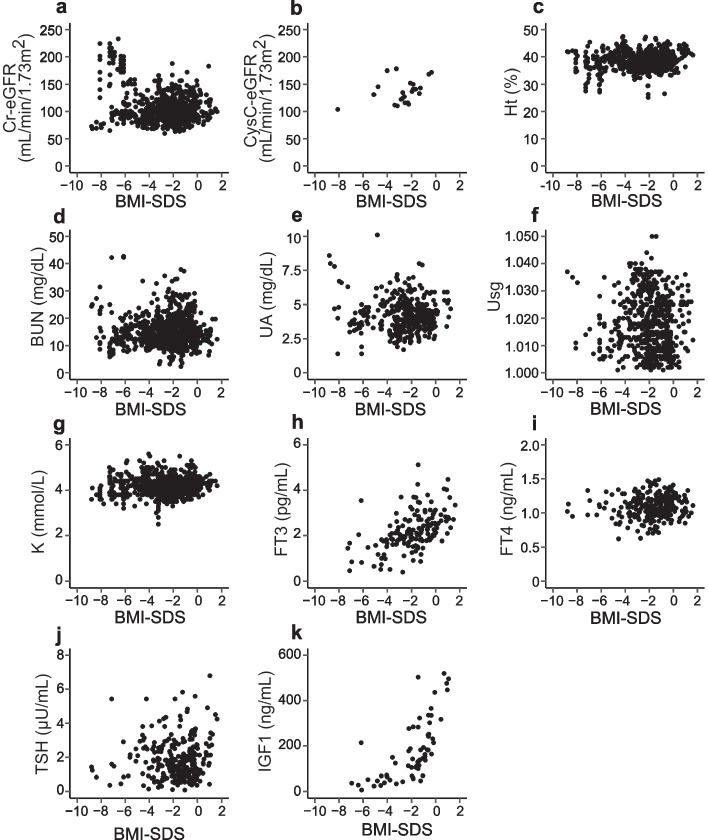
Methods: The data of 39 patients diagnosed with AN between January 2005 and December 2023 was available for study. The characteristics of patients at the lowest and highest body mass index standard deviation score (BMI-SDS) were examined. Data on the parameters Cr-eGFR, CysC-eGFR, dehydration markers, potassium (K), and hormonal data and BMI-SDS were assessed during the treatment course to evaluate the correlations in these parameters. Blood hematocrit, uric acid (UA), blood urine nitrogen (BUN) level, and urine specific gravity were adopted as dehydration markers; FT3, free thyroxine, thyroid stimulating hormone, and insulin-like growth factor were adopted as hormonal data. Cr-eGFR and simultaneously evaluated dehydration markers, K, or hormonal data were extracted and correlations associated with the changes in BMI-SDS were examined. Furthermore, Cr-eGFR and simultaneously assessed CysC-eGFR were compared.
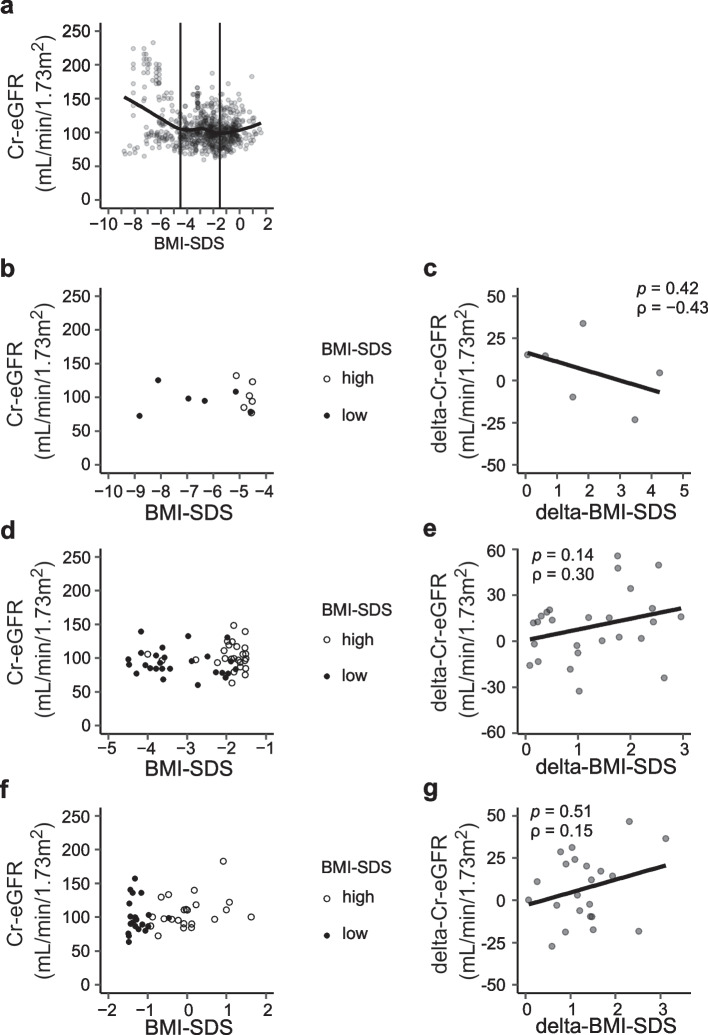
Results: When the BMI-SDS was at the lowest value, low-FT3 syndrome was shown. Severe hypokalemia was not found in our study. A linear relation was not found between Cr-eGFR and BMI-SDS. A statistically significant correlation was found between Cr-eGFR and FT3 (p = 0.0025). Among the dehydration markers, statistically significant correlations were found between Cr-eGFR and BUN or UA. The difference between Cr-eGFR and CysC-eGFR was prominent, and CysC-eGFR showed much higher values.
Conclusions: Our data indicates that low-FT3 syndrome and dehydration were related to the renal function of our patients with AN. Furthermore, our data suggest that caution is needed in the interpretation of kidney function evaluation when using CysC-eGFR in cases of AN.
期刊介绍:
BioPsychoSocial Medicine is an open access, peer-reviewed online journal that encompasses all aspects of the interrelationships between the biological, psychological, social, and behavioral factors of health and illness. BioPsychoSocial Medicine is the official journal of the Japanese Society of Psychosomatic Medicine, and publishes research on psychosomatic disorders and diseases that are characterized by objective organic changes and/or functional changes that could be induced, progressed, aggravated, or exacerbated by psychological, social, and/or behavioral factors and their associated psychosomatic treatments.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
