{"title":"局部晚期宫颈癌伴盆腔淋巴结转移的主动脉旁和盆腔淋巴结切除术。","authors":"Wei Jiang, Mei-Ling Zhong, Su-Lan Wang, Yan Chen, Ya-Nan Wang, Si-Yuan Zeng, Mei-Rong Liang","doi":"10.1186/s12957-024-03540-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study sought to explore the efficiency of para-aortic and pelvic lymphadenectomy in the treatment of locally advanced cervical cancer (LACC) with pelvic lymph node (PLN) metastasis.</p><p><strong>Methods: </strong>A total of 171 LACC patients with imaging-confirmed pelvic lymph node metastasis were included in this study. These patients were divided into two groups: the surgical staging group, comprising 58 patients who had received para-aortic and pelvic lymphadenectomy (surgical staging) along with concurrent chemoradiation therapy (CCRT), and the imaging staging group, comprising 113 patients who had received only CCRT. The two groups' progression-free survival (PFS), overall survival (OS) and treatment-related complications were compared.</p><p><strong>Results: </strong>The surgical staging group started radiotherapy 10.2 days (range 9-12 days) later than the imaging staging group. The overall incidence of lymphatic cysts was 9.30%. In the surgical staging group, para-aortic lymph node metastasis was identified in 34.48% (20/58) of patients, while pathology-negative PLN was observed in 12.07% (7/58). Over a median follow-up period of 52 months, no significant differences in PFS and OS rates were found between the two groups (p > 0.05). Subgroup analysis of patients with lymph node diameters of ≥ 1.5 cm revealed a five-year PFS rate of 75.0% and an OS rate of 80.0% in the surgical staging group, compared to 41.5% and 50.1% in the imaging staging group, respectively, showing statistically significant differences (p = 0.022, HR:0.34 [0.13, 0.90] and p = 0.038, HR: 0.34 [0.12,0.94], respectively for PFS and OS). Additionally, in patients with two or more metastatic lymph nodes, the five-year PFS and OS rates were 69.2% and 73.1% in the surgical staging group, versus 41.0% and 48.4% in the imaging staging group, with these differences also being statistically significant (p = 0.025, HR: 0.41[0.19,0.93] and p = 0.046, HR: 0.42[0.18,0.98], respectively).</p><p><strong>Conclusion: </strong>Performing surgical staging before CCRT is safe and delivers accurate lymph node details crucial for tailoring radiotherapy. This approach merits further investigation, particularly in women with pelvic lymph nodes measuring 1.5 cm or more in diameter or patients with two or more imaging-positive PLNs.</p>","PeriodicalId":23856,"journal":{"name":"World Journal of Surgical Oncology","volume":"22 1","pages":"262"},"PeriodicalIF":2.5000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11440892/pdf/","citationCount":"0","resultStr":"{\"title\":\"Para-aortic and pelvic lymphadenectomy in locally advanced cervical cancer with pelvic lymph node metastasis.\",\"authors\":\"Wei Jiang, Mei-Ling Zhong, Su-Lan Wang, Yan Chen, Ya-Nan Wang, Si-Yuan Zeng, Mei-Rong Liang\",\"doi\":\"10.1186/s12957-024-03540-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study sought to explore the efficiency of para-aortic and pelvic lymphadenectomy in the treatment of locally advanced cervical cancer (LACC) with pelvic lymph node (PLN) metastasis.</p><p><strong>Methods: </strong>A total of 171 LACC patients with imaging-confirmed pelvic lymph node metastasis were included in this study. These patients were divided into two groups: the surgical staging group, comprising 58 patients who had received para-aortic and pelvic lymphadenectomy (surgical staging) along with concurrent chemoradiation therapy (CCRT), and the imaging staging group, comprising 113 patients who had received only CCRT. The two groups' progression-free survival (PFS), overall survival (OS) and treatment-related complications were compared.</p><p><strong>Results: </strong>The surgical staging group started radiotherapy 10.2 days (range 9-12 days) later than the imaging staging group. The overall incidence of lymphatic cysts was 9.30%. In the surgical staging group, para-aortic lymph node metastasis was identified in 34.48% (20/58) of patients, while pathology-negative PLN was observed in 12.07% (7/58). Over a median follow-up period of 52 months, no significant differences in PFS and OS rates were found between the two groups (p > 0.05). Subgroup analysis of patients with lymph node diameters of ≥ 1.5 cm revealed a five-year PFS rate of 75.0% and an OS rate of 80.0% in the surgical staging group, compared to 41.5% and 50.1% in the imaging staging group, respectively, showing statistically significant differences (p = 0.022, HR:0.34 [0.13, 0.90] and p = 0.038, HR: 0.34 [0.12,0.94], respectively for PFS and OS). Additionally, in patients with two or more metastatic lymph nodes, the five-year PFS and OS rates were 69.2% and 73.1% in the surgical staging group, versus 41.0% and 48.4% in the imaging staging group, with these differences also being statistically significant (p = 0.025, HR: 0.41[0.19,0.93] and p = 0.046, HR: 0.42[0.18,0.98], respectively).</p><p><strong>Conclusion: </strong>Performing surgical staging before CCRT is safe and delivers accurate lymph node details crucial for tailoring radiotherapy. This approach merits further investigation, particularly in women with pelvic lymph nodes measuring 1.5 cm or more in diameter or patients with two or more imaging-positive PLNs.</p>\",\"PeriodicalId\":23856,\"journal\":{\"name\":\"World Journal of Surgical Oncology\",\"volume\":\"22 1\",\"pages\":\"262\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11440892/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Surgical Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12957-024-03540-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Surgical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12957-024-03540-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Para-aortic and pelvic lymphadenectomy in locally advanced cervical cancer with pelvic lymph node metastasis.
Objective: This study sought to explore the efficiency of para-aortic and pelvic lymphadenectomy in the treatment of locally advanced cervical cancer (LACC) with pelvic lymph node (PLN) metastasis.
Methods: A total of 171 LACC patients with imaging-confirmed pelvic lymph node metastasis were included in this study. These patients were divided into two groups: the surgical staging group, comprising 58 patients who had received para-aortic and pelvic lymphadenectomy (surgical staging) along with concurrent chemoradiation therapy (CCRT), and the imaging staging group, comprising 113 patients who had received only CCRT. The two groups' progression-free survival (PFS), overall survival (OS) and treatment-related complications were compared.
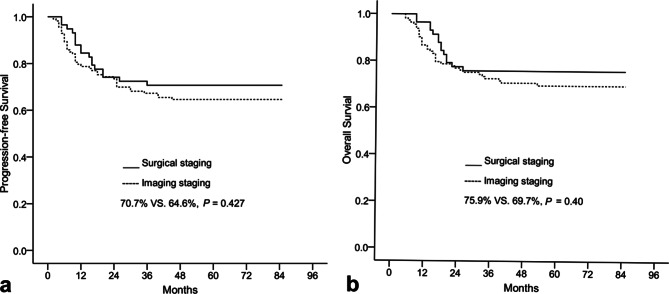
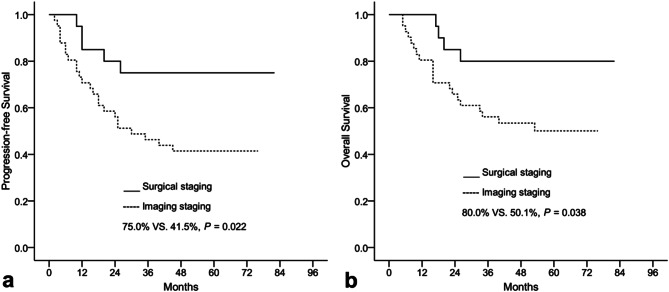
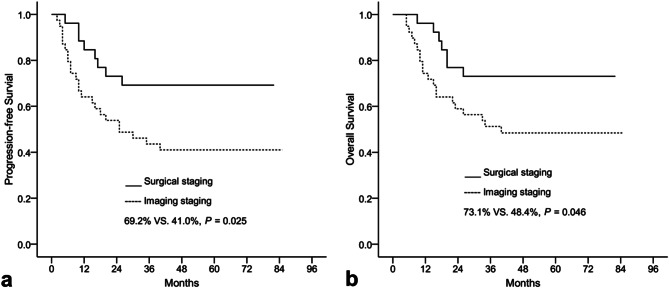
Results: The surgical staging group started radiotherapy 10.2 days (range 9-12 days) later than the imaging staging group. The overall incidence of lymphatic cysts was 9.30%. In the surgical staging group, para-aortic lymph node metastasis was identified in 34.48% (20/58) of patients, while pathology-negative PLN was observed in 12.07% (7/58). Over a median follow-up period of 52 months, no significant differences in PFS and OS rates were found between the two groups (p > 0.05). Subgroup analysis of patients with lymph node diameters of ≥ 1.5 cm revealed a five-year PFS rate of 75.0% and an OS rate of 80.0% in the surgical staging group, compared to 41.5% and 50.1% in the imaging staging group, respectively, showing statistically significant differences (p = 0.022, HR:0.34 [0.13, 0.90] and p = 0.038, HR: 0.34 [0.12,0.94], respectively for PFS and OS). Additionally, in patients with two or more metastatic lymph nodes, the five-year PFS and OS rates were 69.2% and 73.1% in the surgical staging group, versus 41.0% and 48.4% in the imaging staging group, with these differences also being statistically significant (p = 0.025, HR: 0.41[0.19,0.93] and p = 0.046, HR: 0.42[0.18,0.98], respectively).
Conclusion: Performing surgical staging before CCRT is safe and delivers accurate lymph node details crucial for tailoring radiotherapy. This approach merits further investigation, particularly in women with pelvic lymph nodes measuring 1.5 cm or more in diameter or patients with two or more imaging-positive PLNs.
期刊介绍:
World Journal of Surgical Oncology publishes articles related to surgical oncology and its allied subjects, such as epidemiology, cancer research, biomarkers, prevention, pathology, radiology, cancer treatment, clinical trials, multimodality treatment and molecular biology. Emphasis is placed on original research articles. The journal also publishes significant clinical case reports, as well as balanced and timely reviews on selected topics.
Oncology is a multidisciplinary super-speciality of which surgical oncology forms an integral component, especially with solid tumors. Surgical oncologists around the world are involved in research extending from detecting the mechanisms underlying the causation of cancer, to its treatment and prevention. The role of a surgical oncologist extends across the whole continuum of care. With continued developments in diagnosis and treatment, the role of a surgical oncologist is ever-changing. Hence, World Journal of Surgical Oncology aims to keep readers abreast with latest developments that will ultimately influence the work of surgical oncologists.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
