Garrett L Healy, Christina M Stuart, Adam R Dyas, Michael R Bronsert, Robert A Meguid, Tochi Anioke, Ahmad M Hider, Richard D Schulick, William G Henderson
{"title":"术后并发症与住院时间之间的关系:美国外科学院国家外科质量改进计划(ACS-NSQIP)登记处对 4495582 名患者进行的大规模观察研究。","authors":"Garrett L Healy, Christina M Stuart, Adam R Dyas, Michael R Bronsert, Robert A Meguid, Tochi Anioke, Ahmad M Hider, Richard D Schulick, William G Henderson","doi":"10.1186/s13037-024-00409-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Precise estimates of risk-adjusted increases in postoperative length of stay (LOS) associated with postoperative complications across a range of complications and operations are not available in the existing literature.</p><p><strong>Methods: </strong>Associations between preoperative characteristics, postoperative complications and postoperative LOS were tested using medians, interquartile ranges, and nonparametric rank sum tests in a retrospective cohort study using the 2005-2018 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) dataset. A negative binomial model was used with postoperative LOS as the dependent variable and preoperative characteristics and postoperative complications as independent variables. The model was applied to estimate each patient's postoperative LOS with and without each postoperative complication to measure the association between each complication and risk-adjusted change in postoperative LOS.</p><p><strong>Results: </strong>A total of 4,495,582 patients were included. After risk-adjustment, occurrence of each postoperative complication was associated with significantly increased postoperative LOS (between + 3.9 and + 20.1 days, p < 0.0001). The longest risk-adjusted postoperative LOS increases were associated with prolonged ventilator use (+ 20.1 days), wound disruption (+ 19.4 days), and acute renal failure (+ 17.1 days).</p><p><strong>Conclusion: </strong>Occurrence of any postoperative complication was associated with increased risk-adjusted postoperative LOS. Degree of increase varied by complication. These data could be useful for patient counseling, allocation of resources, discharge planning, and quality improvement efforts.</p>","PeriodicalId":46782,"journal":{"name":"Patient Safety in Surgery","volume":"18 1","pages":"29"},"PeriodicalIF":3.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11443812/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between postoperative complications and hospital length of stay: a large-scale observational study of 4,495,582 patients in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) registry.\",\"authors\":\"Garrett L Healy, Christina M Stuart, Adam R Dyas, Michael R Bronsert, Robert A Meguid, Tochi Anioke, Ahmad M Hider, Richard D Schulick, William G Henderson\",\"doi\":\"10.1186/s13037-024-00409-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Precise estimates of risk-adjusted increases in postoperative length of stay (LOS) associated with postoperative complications across a range of complications and operations are not available in the existing literature.</p><p><strong>Methods: </strong>Associations between preoperative characteristics, postoperative complications and postoperative LOS were tested using medians, interquartile ranges, and nonparametric rank sum tests in a retrospective cohort study using the 2005-2018 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) dataset. A negative binomial model was used with postoperative LOS as the dependent variable and preoperative characteristics and postoperative complications as independent variables. The model was applied to estimate each patient's postoperative LOS with and without each postoperative complication to measure the association between each complication and risk-adjusted change in postoperative LOS.</p><p><strong>Results: </strong>A total of 4,495,582 patients were included. After risk-adjustment, occurrence of each postoperative complication was associated with significantly increased postoperative LOS (between + 3.9 and + 20.1 days, p < 0.0001). The longest risk-adjusted postoperative LOS increases were associated with prolonged ventilator use (+ 20.1 days), wound disruption (+ 19.4 days), and acute renal failure (+ 17.1 days).</p><p><strong>Conclusion: </strong>Occurrence of any postoperative complication was associated with increased risk-adjusted postoperative LOS. Degree of increase varied by complication. These data could be useful for patient counseling, allocation of resources, discharge planning, and quality improvement efforts.</p>\",\"PeriodicalId\":46782,\"journal\":{\"name\":\"Patient Safety in Surgery\",\"volume\":\"18 1\",\"pages\":\"29\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11443812/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Patient Safety in Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13037-024-00409-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Safety in Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13037-024-00409-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
背景:现有文献中还没有关于术后并发症导致的术后住院时间(LOS)增加的风险调整后的精确估计:方法:在一项回顾性队列研究中,使用 2005-2018 年美国外科学院国家外科质量改进计划(ACS-NSQIP)数据集,使用中位数、四分位间范围和非参数秩和检验对术前特征、术后并发症和术后住院时间之间的相关性进行了检验。采用负二项模型,以术后 LOS 为因变量,术前特征和术后并发症为自变量。该模型用于估算每位患者在出现和未出现每种术后并发症时的术后住院时间,以衡量每种并发症与风险调整后的术后住院时间变化之间的关联:结果:共纳入 4495582 名患者。经过风险调整后,每种术后并发症的发生都与术后 LOS 的显著增加有关(介于 + 3.9 天和 + 20.1 天之间,p 结论:每种术后并发症的发生都与术后 LOS 的显著增加有关(介于 + 3.9 天和 + 20.1 天之间,p 结论):任何一种术后并发症的发生都与风险调整后的术后 LOS 增加有关。不同并发症导致的延长程度不同。这些数据对患者咨询、资源分配、出院计划和质量改进工作很有帮助。
Association between postoperative complications and hospital length of stay: a large-scale observational study of 4,495,582 patients in the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) registry.
Background: Precise estimates of risk-adjusted increases in postoperative length of stay (LOS) associated with postoperative complications across a range of complications and operations are not available in the existing literature.
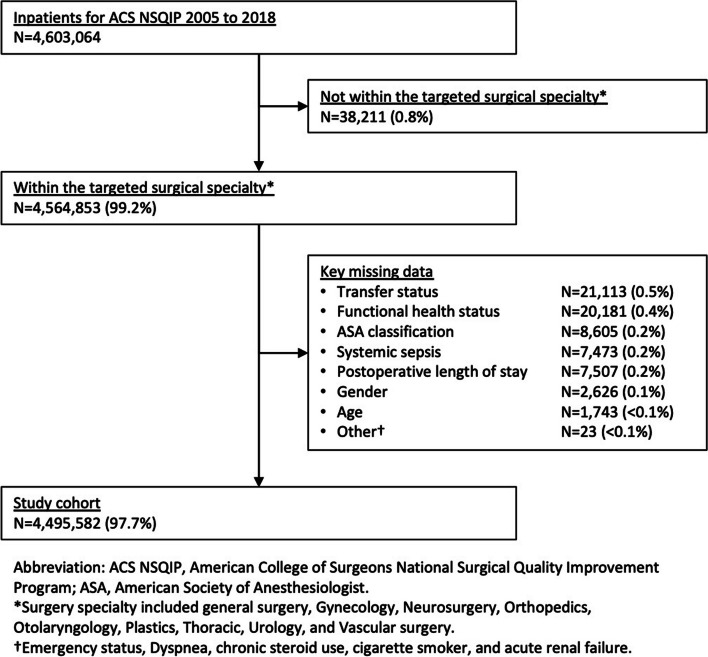
Methods: Associations between preoperative characteristics, postoperative complications and postoperative LOS were tested using medians, interquartile ranges, and nonparametric rank sum tests in a retrospective cohort study using the 2005-2018 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) dataset. A negative binomial model was used with postoperative LOS as the dependent variable and preoperative characteristics and postoperative complications as independent variables. The model was applied to estimate each patient's postoperative LOS with and without each postoperative complication to measure the association between each complication and risk-adjusted change in postoperative LOS.
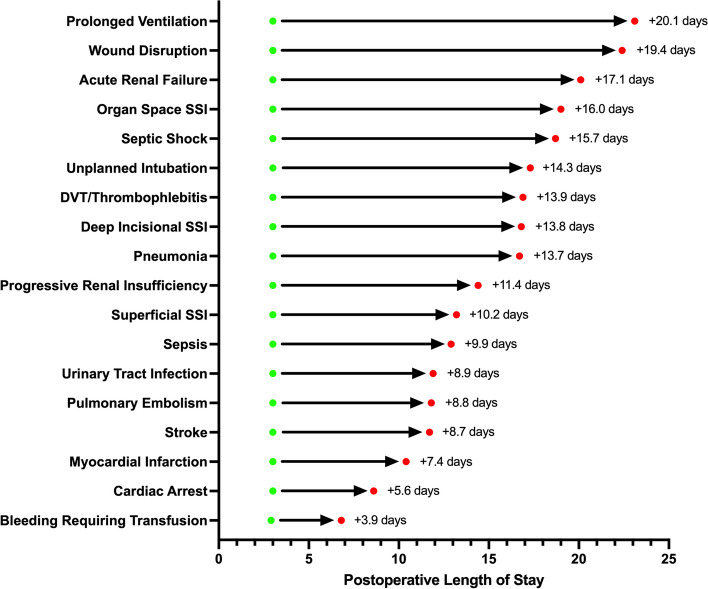
Results: A total of 4,495,582 patients were included. After risk-adjustment, occurrence of each postoperative complication was associated with significantly increased postoperative LOS (between + 3.9 and + 20.1 days, p < 0.0001). The longest risk-adjusted postoperative LOS increases were associated with prolonged ventilator use (+ 20.1 days), wound disruption (+ 19.4 days), and acute renal failure (+ 17.1 days).
Conclusion: Occurrence of any postoperative complication was associated with increased risk-adjusted postoperative LOS. Degree of increase varied by complication. These data could be useful for patient counseling, allocation of resources, discharge planning, and quality improvement efforts.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
