Donatas Opulskis, Imam T P Ritonga, Philipp Franke, Martin J Austermann, Marco Virgilio Usai
{"title":"使用分支EVAR治疗并arenal主动脉瘤和重要肾动脉:货架上的另一种工具?病例报告。","authors":"Donatas Opulskis, Imam T P Ritonga, Philipp Franke, Martin J Austermann, Marco Virgilio Usai","doi":"10.1177/15385744241290011","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We present the case of a 58-year-old male patient referred to our department from a smaller facility for further evaluation and treatment strategy regarding the choice between open or endovascular surgery. The patient was diagnosed with a 6 cm asymptomatic juxtarenal aortic aneurysm and a 5 mm diameter accessory renal artery (ARA) supplying the lower half of left kidney. Further diagnostic assessments indicated that the left ARA was perfusing over 40% of the left kidney.</p><p><strong>Methods: </strong>Given the patient's significant pre-existing medical conditions and elevated perioperative risk, the decision was made to proceed with minimally invasive endovascular surgery using a custom-made 5-branches stent graft (BEVAR).</p><p><strong>Results: </strong>In the early postoperative period, the patient reported left flank pain. A subsequent CT scan identified a partial infarction in the left kidney due to the occlusion of an early small branch from the upper left renal artery. However, laboratory results showed no significant change in renal function compared to preoperative values. The patient was discharged 6 days post-surgery, with no additional complications observed during the early postoperative period.</p><p><strong>Conclusion: </strong>This case report demonstrates that BEVAR is acceptable technique with satisfactory early postoperative outcomes for treating juxtarenal aortic aneurysms with an accessory renal artery in patients who are high-risk candidates for open repair and anatomically unsuitable for FEVAR or Ch-EVAR procedures.</p>","PeriodicalId":94265,"journal":{"name":"Vascular and endovascular surgery","volume":" ","pages":"303-308"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11804137/pdf/","citationCount":"0","resultStr":"{\"title\":\"Use of Branched EVAR in Treatment of Juxtarenal Aortic Aneurysm and Essential Accessory Renal Artery: Another Tool on the Shelf? A Case Report.\",\"authors\":\"Donatas Opulskis, Imam T P Ritonga, Philipp Franke, Martin J Austermann, Marco Virgilio Usai\",\"doi\":\"10.1177/15385744241290011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We present the case of a 58-year-old male patient referred to our department from a smaller facility for further evaluation and treatment strategy regarding the choice between open or endovascular surgery. The patient was diagnosed with a 6 cm asymptomatic juxtarenal aortic aneurysm and a 5 mm diameter accessory renal artery (ARA) supplying the lower half of left kidney. Further diagnostic assessments indicated that the left ARA was perfusing over 40% of the left kidney.</p><p><strong>Methods: </strong>Given the patient's significant pre-existing medical conditions and elevated perioperative risk, the decision was made to proceed with minimally invasive endovascular surgery using a custom-made 5-branches stent graft (BEVAR).</p><p><strong>Results: </strong>In the early postoperative period, the patient reported left flank pain. A subsequent CT scan identified a partial infarction in the left kidney due to the occlusion of an early small branch from the upper left renal artery. However, laboratory results showed no significant change in renal function compared to preoperative values. The patient was discharged 6 days post-surgery, with no additional complications observed during the early postoperative period.</p><p><strong>Conclusion: </strong>This case report demonstrates that BEVAR is acceptable technique with satisfactory early postoperative outcomes for treating juxtarenal aortic aneurysms with an accessory renal artery in patients who are high-risk candidates for open repair and anatomically unsuitable for FEVAR or Ch-EVAR procedures.</p>\",\"PeriodicalId\":94265,\"journal\":{\"name\":\"Vascular and endovascular surgery\",\"volume\":\" \",\"pages\":\"303-308\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11804137/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vascular and endovascular surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/15385744241290011\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular and endovascular surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/15385744241290011","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Use of Branched EVAR in Treatment of Juxtarenal Aortic Aneurysm and Essential Accessory Renal Artery: Another Tool on the Shelf? A Case Report.
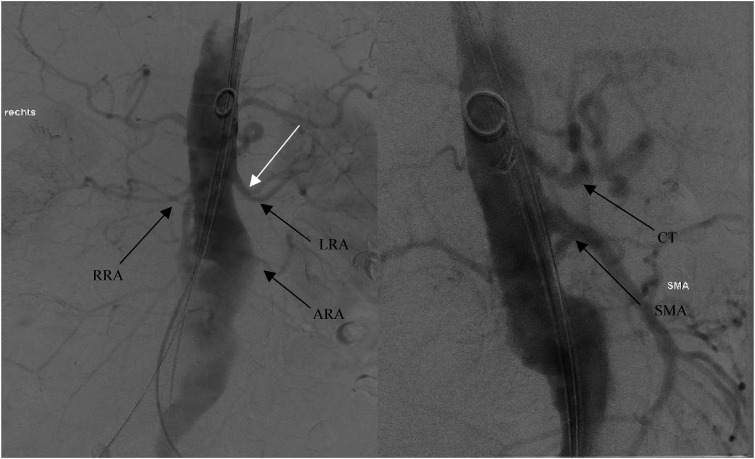
Objective: We present the case of a 58-year-old male patient referred to our department from a smaller facility for further evaluation and treatment strategy regarding the choice between open or endovascular surgery. The patient was diagnosed with a 6 cm asymptomatic juxtarenal aortic aneurysm and a 5 mm diameter accessory renal artery (ARA) supplying the lower half of left kidney. Further diagnostic assessments indicated that the left ARA was perfusing over 40% of the left kidney.
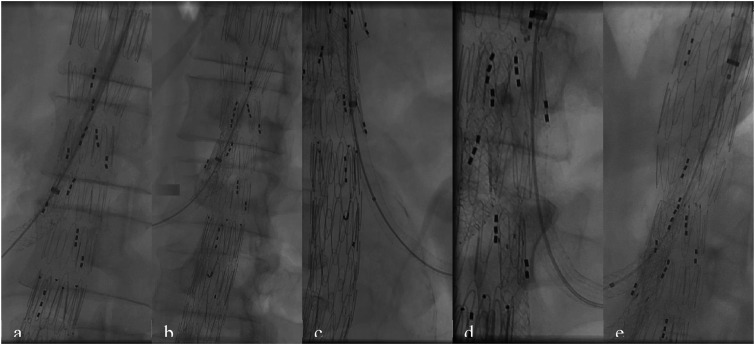
Methods: Given the patient's significant pre-existing medical conditions and elevated perioperative risk, the decision was made to proceed with minimally invasive endovascular surgery using a custom-made 5-branches stent graft (BEVAR).
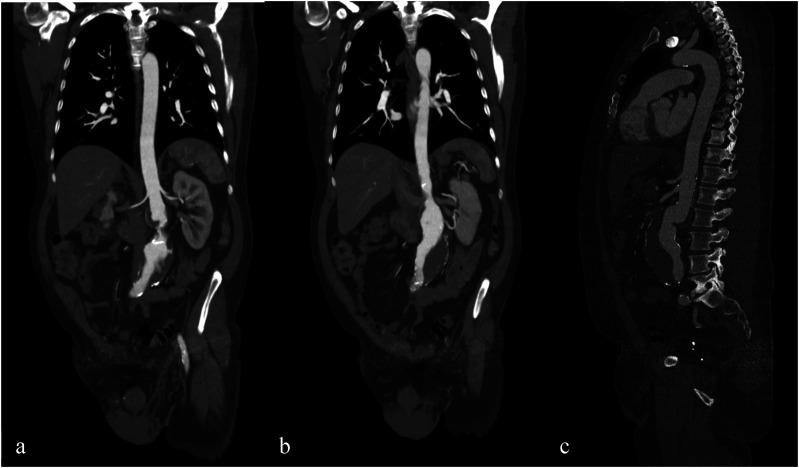
Results: In the early postoperative period, the patient reported left flank pain. A subsequent CT scan identified a partial infarction in the left kidney due to the occlusion of an early small branch from the upper left renal artery. However, laboratory results showed no significant change in renal function compared to preoperative values. The patient was discharged 6 days post-surgery, with no additional complications observed during the early postoperative period.
Conclusion: This case report demonstrates that BEVAR is acceptable technique with satisfactory early postoperative outcomes for treating juxtarenal aortic aneurysms with an accessory renal artery in patients who are high-risk candidates for open repair and anatomically unsuitable for FEVAR or Ch-EVAR procedures.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
