João Sérgio Neves, Ana Rita Leite, Robert J. Mentz, Rury R. Holman, Faiez Zannad, Javed Butler, Milton Packer, João Pedro Ferreira
{"title":"根据射血分数评估 2 型糖尿病患者使用艾塞那肽治疗心血管疾病的效果:EXSCEL试验","authors":"João Sérgio Neves, Ana Rita Leite, Robert J. Mentz, Rury R. Holman, Faiez Zannad, Javed Butler, Milton Packer, João Pedro Ferreira","doi":"10.1002/ejhf.3478","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>Glucagon-like peptide-1 receptor agonists reduce major adverse cardiovascular events (MACE) and cardiovascular mortality in people with type 2 diabetes (T2D). However, previous studies suggest the effects on heart failure outcomes vary according to left ventricular ejection fraction (LVEF). We aimed to evaluate the effects of exenatide on cardiovascular events according to LVEF in people with T2D.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>Post-hoc analysis of the Exenatide Study of Cardiovascular Event Lowering (EXSCEL) trial evaluating the effects of once-weekly exenatide (EQW) versus placebo on cardiovascular outcomes according to baseline LVEF (<40% or ≥40%). Outcomes were also evaluated according to New York Heart Association (NYHA) class and obesity. The main outcome was hospitalization for heart failure (HHF). A treatment-by-LVEF interaction was used. In EXSCEL (<i>n</i> = 14 752), 4749 participants had LVEF available at baseline; 455 (10%) with LVEF <40%, 4294 (90%) with LVEF ≥40%. LVEF modified the EQW effect on hHF: hazard ratio (HR) = 1.52 (95% confidence interval [CI] = 0.95–2.43) in participants with LVEF < 40% and HR = 0.74 (95% CI = 0.55–1.01) in those with LVEF ≥ 40% (<i>p</i>-interaction = 0.012). No significant treatment-by-LVEF interactions (<i>p</i>-interaction >0.10) were observed for MACE, cardiovascular death or all-cause mortality. The risk of HHF was also modified by baseline NYHA class (HR 0.91, 95% CI 0.65–1.27 for NYHA class I/II; HR 1.84, 95% CI 0.95–3.59 for NYHA class III/IV; <i>p</i>-interaction = 0.062), mostly driven by the LVEF <40% subgroup. Obesity did not modify the effects of EQW on HHF.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>The EQW effect on HHF was influenced by LVEF, with a potentially decreased risk in participants with LVEF ≥40% and increased risk in those with LVEF <40%. The risk of HHF was particularly high in participants with LVEF <40% and NYHA class III/IV. LVEF did not modify the effect of EQW on atherosclerotic outcomes.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"27 3","pages":"540-551"},"PeriodicalIF":10.8000,"publicationDate":"2024-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Cardiovascular outcomes with exenatide in type 2 diabetes according to ejection fraction: The EXSCEL trial\",\"authors\":\"João Sérgio Neves, Ana Rita Leite, Robert J. Mentz, Rury R. Holman, Faiez Zannad, Javed Butler, Milton Packer, João Pedro Ferreira\",\"doi\":\"10.1002/ejhf.3478\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Glucagon-like peptide-1 receptor agonists reduce major adverse cardiovascular events (MACE) and cardiovascular mortality in people with type 2 diabetes (T2D). However, previous studies suggest the effects on heart failure outcomes vary according to left ventricular ejection fraction (LVEF). We aimed to evaluate the effects of exenatide on cardiovascular events according to LVEF in people with T2D.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>Post-hoc analysis of the Exenatide Study of Cardiovascular Event Lowering (EXSCEL) trial evaluating the effects of once-weekly exenatide (EQW) versus placebo on cardiovascular outcomes according to baseline LVEF (<40% or ≥40%). Outcomes were also evaluated according to New York Heart Association (NYHA) class and obesity. The main outcome was hospitalization for heart failure (HHF). A treatment-by-LVEF interaction was used. In EXSCEL (<i>n</i> = 14 752), 4749 participants had LVEF available at baseline; 455 (10%) with LVEF <40%, 4294 (90%) with LVEF ≥40%. LVEF modified the EQW effect on hHF: hazard ratio (HR) = 1.52 (95% confidence interval [CI] = 0.95–2.43) in participants with LVEF < 40% and HR = 0.74 (95% CI = 0.55–1.01) in those with LVEF ≥ 40% (<i>p</i>-interaction = 0.012). No significant treatment-by-LVEF interactions (<i>p</i>-interaction >0.10) were observed for MACE, cardiovascular death or all-cause mortality. The risk of HHF was also modified by baseline NYHA class (HR 0.91, 95% CI 0.65–1.27 for NYHA class I/II; HR 1.84, 95% CI 0.95–3.59 for NYHA class III/IV; <i>p</i>-interaction = 0.062), mostly driven by the LVEF <40% subgroup. Obesity did not modify the effects of EQW on HHF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>The EQW effect on HHF was influenced by LVEF, with a potentially decreased risk in participants with LVEF ≥40% and increased risk in those with LVEF <40%. The risk of HHF was particularly high in participants with LVEF <40% and NYHA class III/IV. LVEF did not modify the effect of EQW on atherosclerotic outcomes.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"27 3\",\"pages\":\"540-551\"},\"PeriodicalIF\":10.8000,\"publicationDate\":\"2024-10-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3478\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3478","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cardiovascular outcomes with exenatide in type 2 diabetes according to ejection fraction: The EXSCEL trial
Aims
Glucagon-like peptide-1 receptor agonists reduce major adverse cardiovascular events (MACE) and cardiovascular mortality in people with type 2 diabetes (T2D). However, previous studies suggest the effects on heart failure outcomes vary according to left ventricular ejection fraction (LVEF). We aimed to evaluate the effects of exenatide on cardiovascular events according to LVEF in people with T2D.
Methods and results
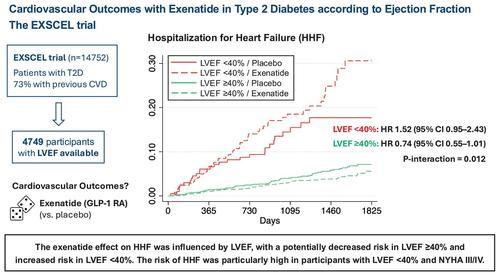
Post-hoc analysis of the Exenatide Study of Cardiovascular Event Lowering (EXSCEL) trial evaluating the effects of once-weekly exenatide (EQW) versus placebo on cardiovascular outcomes according to baseline LVEF (<40% or ≥40%). Outcomes were also evaluated according to New York Heart Association (NYHA) class and obesity. The main outcome was hospitalization for heart failure (HHF). A treatment-by-LVEF interaction was used. In EXSCEL (n = 14 752), 4749 participants had LVEF available at baseline; 455 (10%) with LVEF <40%, 4294 (90%) with LVEF ≥40%. LVEF modified the EQW effect on hHF: hazard ratio (HR) = 1.52 (95% confidence interval [CI] = 0.95–2.43) in participants with LVEF < 40% and HR = 0.74 (95% CI = 0.55–1.01) in those with LVEF ≥ 40% (p-interaction = 0.012). No significant treatment-by-LVEF interactions (p-interaction >0.10) were observed for MACE, cardiovascular death or all-cause mortality. The risk of HHF was also modified by baseline NYHA class (HR 0.91, 95% CI 0.65–1.27 for NYHA class I/II; HR 1.84, 95% CI 0.95–3.59 for NYHA class III/IV; p-interaction = 0.062), mostly driven by the LVEF <40% subgroup. Obesity did not modify the effects of EQW on HHF.
Conclusions
The EQW effect on HHF was influenced by LVEF, with a potentially decreased risk in participants with LVEF ≥40% and increased risk in those with LVEF <40%. The risk of HHF was particularly high in participants with LVEF <40% and NYHA class III/IV. LVEF did not modify the effect of EQW on atherosclerotic outcomes.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
