{"title":"Watson-Jones 前外侧入路在治疗皮普金 II 型骨折脱位中的相关性:病例报告和文献综述。","authors":"Nazim Sifi, Ryad Bouguenna","doi":"10.20408/jti.2024.0004","DOIUrl":null,"url":null,"abstract":"<p><p>Femoral head fractures with associated hip dislocations substantially impact the functional prognosis of the hip joint and present a surgical challenge. The surgeon must select a safe approach that enables osteosynthesis of the fracture while also preserving the vascularization of the femoral head. The optimal surgical approach for these injuries remains a topic of debate. A 44-year-old woman was involved in a road traffic accident, which resulted in a posterior iliac dislocation of the hip associated with a Pipkin type II fracture of the femoral head. Given the size of the detached fragment and the risk of incarceration preventing reduction, we opted against attempting external orthopedic reduction maneuvers. Instead, we chose to perform open reduction and internal fixation using the Watson-Jones anterolateral approach. This involved navigating between the retracted tensor fascia lata muscle, positioned medially, and the gluteus medius and minimus muscles, situated laterally. During radiological and clinical follow-up visits extending to postoperative month 15, the patient showed no signs of avascular necrosis of the femoral head, progression toward coxarthrosis, or heterotopic ossification. The Watson-Jones anterolateral approach is a straightforward intermuscular and internervous surgical procedure. This method provides excellent exposure of the femoral head, preserves its primary vascularization, allows for anterior dislocation, and facilitates the anatomical reduction and fixation of the fracture.</p>","PeriodicalId":52698,"journal":{"name":"Journal of Trauma and Injury","volume":"37 2","pages":"161-165"},"PeriodicalIF":0.6000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11309222/pdf/","citationCount":"0","resultStr":"{\"title\":\"Relevance of the Watson-Jones anterolateral approach in the management of Pipkin type II fracture-dislocation: a case report and literature review.\",\"authors\":\"Nazim Sifi, Ryad Bouguenna\",\"doi\":\"10.20408/jti.2024.0004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Femoral head fractures with associated hip dislocations substantially impact the functional prognosis of the hip joint and present a surgical challenge. The surgeon must select a safe approach that enables osteosynthesis of the fracture while also preserving the vascularization of the femoral head. The optimal surgical approach for these injuries remains a topic of debate. A 44-year-old woman was involved in a road traffic accident, which resulted in a posterior iliac dislocation of the hip associated with a Pipkin type II fracture of the femoral head. Given the size of the detached fragment and the risk of incarceration preventing reduction, we opted against attempting external orthopedic reduction maneuvers. Instead, we chose to perform open reduction and internal fixation using the Watson-Jones anterolateral approach. This involved navigating between the retracted tensor fascia lata muscle, positioned medially, and the gluteus medius and minimus muscles, situated laterally. During radiological and clinical follow-up visits extending to postoperative month 15, the patient showed no signs of avascular necrosis of the femoral head, progression toward coxarthrosis, or heterotopic ossification. The Watson-Jones anterolateral approach is a straightforward intermuscular and internervous surgical procedure. This method provides excellent exposure of the femoral head, preserves its primary vascularization, allows for anterior dislocation, and facilitates the anatomical reduction and fixation of the fracture.</p>\",\"PeriodicalId\":52698,\"journal\":{\"name\":\"Journal of Trauma and Injury\",\"volume\":\"37 2\",\"pages\":\"161-165\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11309222/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Trauma and Injury\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20408/jti.2024.0004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/6/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Trauma and Injury","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20408/jti.2024.0004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/17 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
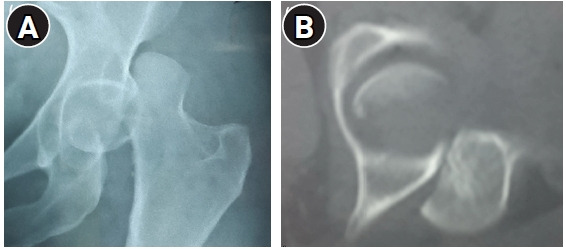
股骨头骨折伴有髋关节脱位会严重影响髋关节的功能预后,是一项外科手术挑战。外科医生必须选择一种安全的方法,既能对骨折进行骨合成,又能保留股骨头的血管。此类损伤的最佳手术方法仍是一个争论不休的话题。一名 44 岁的女性在一次道路交通事故中导致髋关节髂后脱位,并伴有股骨头皮普金 II 型骨折。考虑到脱出碎片的大小以及嵌顿阻碍复位的风险,我们决定不尝试外部矫形复位手法。相反,我们选择使用沃森-琼斯(Watson-Jones)前外侧入路进行切开复位和内固定。这需要在位于内侧的牵张筋膜肌和位于外侧的臀中肌和臀小肌之间穿梭。在术后第15个月的放射学和临床随访中,患者没有出现股骨头血管性坏死、髋关节病变或异位骨化的迹象。Watson-Jones 前外侧入路是一种直接的肌间和颈内手术方法。这种方法能很好地暴露股骨头,保留其主要血管,允许股骨头前脱位,有利于骨折的解剖复位和固定。
Relevance of the Watson-Jones anterolateral approach in the management of Pipkin type II fracture-dislocation: a case report and literature review.
Femoral head fractures with associated hip dislocations substantially impact the functional prognosis of the hip joint and present a surgical challenge. The surgeon must select a safe approach that enables osteosynthesis of the fracture while also preserving the vascularization of the femoral head. The optimal surgical approach for these injuries remains a topic of debate. A 44-year-old woman was involved in a road traffic accident, which resulted in a posterior iliac dislocation of the hip associated with a Pipkin type II fracture of the femoral head. Given the size of the detached fragment and the risk of incarceration preventing reduction, we opted against attempting external orthopedic reduction maneuvers. Instead, we chose to perform open reduction and internal fixation using the Watson-Jones anterolateral approach. This involved navigating between the retracted tensor fascia lata muscle, positioned medially, and the gluteus medius and minimus muscles, situated laterally. During radiological and clinical follow-up visits extending to postoperative month 15, the patient showed no signs of avascular necrosis of the femoral head, progression toward coxarthrosis, or heterotopic ossification. The Watson-Jones anterolateral approach is a straightforward intermuscular and internervous surgical procedure. This method provides excellent exposure of the femoral head, preserves its primary vascularization, allows for anterior dislocation, and facilitates the anatomical reduction and fixation of the fracture.





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
