Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min
{"title":"以预后为导向的腹膜后脂肪肉瘤分子亚型","authors":"Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min","doi":"10.1002/ctm2.70050","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Retroperitoneal liposarcoma (RPLS) is an extremely rare malignant tumour.<span><sup>1</sup></span> It is largely understudied with unknown risk factors and limited treatment options. The rapid development of next-generation sequencing technology has brought the diagnosis and treatment of neoplastic diseases to the era of precision medicine.<span><sup>2</sup></span> It provided detailed RNA-seq information for the prognosis and prediction of different therapies and guided the crucial clinical decision-making processes throughout the treatment.<span><sup>3</sup></span> Here, we aim to develop prognosis-oriented molecular subtyping of RPLS and further provide novel treatment strategies for RPLS patients (Figure 1A). This work fundamentally differs from our previous reports.<span><sup>4</sup></span> It focuses on prognostic genes rather than differential genes, employing Weighted Gene Network Analysis and nonnegative matrix factorization (NMF) algorithms to achieve a more refined molecular classification of RPLS. By selecting and validating representative molecular biomarkers for each subtype, we have further streamlined the classification system for clinical application. Additionally, this classification system elucidates how the molecular biological characteristics of the different subtypes influence distinct clinical prognoses.</p><p>To construct prognosis-oriented RPLS molecular subtypes, we first identify the prognostic genes in our training cohort based on univariate cox regression (<i>N</i> = 80, Table 1; Tables S1 and S2). The regression analysis pipeline was conducted with the R package “survival” (Supporting Information Material and methods). A total of 3550 genes were associated with OS and DFS (<i>p </i>< .05; Figure 1B), and the top 10 genes of HR > 1 and HR < 1 were shown in Figure 1C. Functional annotation revealed these genes were enriched in the cell cycle, TGFβ-signalling pathway, angiopoietin, and cellular senescence (Figure 1D–F). We then functionally clustered 3550 prognostic genes by WGCNA (Figure S1) and selected the top 20 genes in each module for NMF grouping. Three RPLS subtypes were significantly distinguished (Figure 1G–H). Log-rank analysis showed that subtype 2 (S2) had the best prognostic outcomes (including OS, <i>p</i> < .0046; DFS, <i>p</i> < .0001) compared with subtype 1 (S1) and subtype 3 (S3), while S3 had the worst prognostic outcomes among them (Figure 2A,B). Functional annotation of characteristic genes showed that “Obesity”, “Overnutrition”, and “<i>PPAR</i> signaling pathway” were mainly enrichment terms of S2 (Figure S2).</p><p>Hallmark gene set of cancer well represents the specific biological processes and states of tumours. We previously revealed the differences in the functional annotation among subtypes. To verify them, hallmark gene sets were scored on patients of each subtype by ssGSEA. We found that metabolism-related pathways, including “adipogenesis” and “bile acid metabolism”, were most strongly associated with S2. This observation is consistent with recent studies that elucidate the role of bile acids in modulating the tumour immune microenvironment, as well as their involvement in lipogenesis, metabolism, and the regulation of tumour proliferation and apoptosis.<span><sup>5-7</sup></span> These findings underscore the critical role of bile acids in tumorigenesis and progression. Proliferation-related pathways, such as “mitotic spindle” and “G2M checkpoint” were the most important biological processes in S3, while immune-related pathways, such as “TNFα”, “IL2-STAT5” and “IFNα and IFNβ response” were mainly enriched in S1 (Figure 2C). Although activation of immune responses can significantly inhibit tumour progression, concomitant upregulation of PI3K-Akt-mTOR and KRAS signalling pathways reduces S1 prognosis.<span><sup>8</sup></span> We also evaluated the tumour microenvironment (TME, using the ESTIMATE algorithm) and clinical signatures (using one-way ANOVA) among three subtypes (Supplementary material and methods), the results showed that S3 had the lowest TME score and smallest tumour size (Figure 2D,E), but had the highest MDM2 expression, Ki67 index and FNCLCC score (Figure 2F,H), the most surgery times (Figure 2I), and the most significant pathological subtype ratio (DDLS/WDLS) among them (Figure 2J). These results demonstrated that the subtypes exhibited distinct biological features connecting the clinical, pathological, and prognostic signatures of RPLS.</p><p>For the NMF classification of RPLS patients, KLF6, ECM2, and LMNB2 were identified as representative biomarkers of S1, S2, and S3, respectively (Figure 2K and Figure S3). We then performed log-rank analysis according to the expression level of the three biomarkers, and the results showed that RPLS patients with high expressed KLF6 and ECM2 had better OS (KLF6: <i>p</i> = .034; ECM2: <i>p</i> = .035; Figure 2L,N) and DFS (KLF6: <i>p</i> = .0096; ECM2: <i>p</i> < .001; Figure 2M,O). However, Patients with high expressed LMNB2 had worse OS (<i>p</i> = .013, Figure 2P) and DFS (<i>p</i> < .001, Figure 2Q). KLF6 and ECM2 were important tumour suppressors in many tumours, they acted a beneficial role by inactivating p38/JNK/ERK signalling and increasing p21 in a p53-independent manner.<span><sup>9, 10</sup></span> LMNB2 is crucial in maintaining the integrity of the nuclear skeleton and participating in cell proliferation, ageing, and DNA damage repair.<span><sup>11</sup></span> It promotes the progression of these tumours by silencing p21, ki67, and caspase3, activating CDCA3, and regulating immune infiltrates.<span><sup>12-14</sup></span> These results suggest that the representative biomarkers are prognostic molecules in nature, which echoes our initial design idea of establishing prognosis-oriented molecular subtypes of RPLS.</p><p>Finally, we validated the representative biomarkers in the Retroperitoneal Sarcoma Registry (RESAR) cohort (<i>N</i> = 174, NCT03838718, Table 1). IHC staining was performed as previously described (Supporting Information Material and Methods) and the representative images with different degrees of expression are shown in Figure 3A. These classifications are derived from a comprehensive evaluation of biomarkers’ expression across all validation cohort samples, with the lowest one-third designated as low expression, the middle one-third as intermediate expression, and the highest one-third as high expression. We found that RPLS patients with higher <i>KLF6</i> and <i>ECM2</i> had better OS (Figure 3B,D) and DFS (Figure 3C,E) than those with lower expression, whereas patients with higher <i>LMNB2</i> had worse OS and DFS than patients with lower expression (Figure 3F,G). It is consistent with our previous findings in our training cohort. To further validate the three-gene-based molecular subtypes, we divided RPLS patients into three subgroups for prognosis analysis according to which biomarker (<i>KLF6</i>, <i>ECM2</i>, and <i>LMNB2</i>) showed the highest expression (Table S3). The <i>ECM2</i> subgroup had the best OS and DFS, whereas the <i>LMNB2</i> subgroup had the poorest OS and DFS (Figure 3H,I). Besides, the highest pathological subtype ratio (DDLS/WDLS), <i>Ki67</i> level, and most surgery times (Figure 3J–L) were observed in the <i>LMNB2</i> subgroup, in accordance with disease progression.</p><p>To sum up, we proposed three RPLS subtypes with IHC-verified biomarkers. The new classification of RPLS revealed distinct biological features and indicated various prognoses. It would be a preliminary but essential effort to bring RPLS treatment to the precision medicine era.</p><p>Conception/design: Li Min, Chenghua Luo; provision of study material or patients: Chenghua Luo, Mengmeng Xiao, Shixiang Ma, Xiaobing Chen; collection and/or assembly of data: Da Qin, Xiangji Li, Fanqin Bu, Yu Zhao; data analysis and interpretation: Xiangji Li, Da Qin, Fanqin Bu; manuscript writing: Mengmeng Xiao, Xiangji Li, Fanqin Bu, Li Min; final approval of manuscript: Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min.</p><p>The authors declare no conflict of interest.</p><p>This work was supported by grants from the Young Elite Scientists Sponsorship Program (2023QNRC001) and the National Natural Science Foundation of China (82073390). The study sponsors had no role in the design and preparation of this manuscript.</p><p>Specimens of RPLS patients were obtained from Peking University International Hospital. The experiments were undertaken with the understanding and written consent of each subject. The study protocol conformed to the standards set by the Declaration of Helsinki and was approved by the Ethics Committee of Peking University International Hospital, Peking University Health Science Center (WA2020RW29).</p><p>All authors have read and approved the manuscript and agree with submission to Clinical and Translational Medicine.</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 10","pages":""},"PeriodicalIF":6.8000,"publicationDate":"2024-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.70050","citationCount":"0","resultStr":"{\"title\":\"Prognosis-oriented molecular subtypes of retroperitoneal liposarcoma\",\"authors\":\"Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min\",\"doi\":\"10.1002/ctm2.70050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Dear Editor,</p><p>Retroperitoneal liposarcoma (RPLS) is an extremely rare malignant tumour.<span><sup>1</sup></span> It is largely understudied with unknown risk factors and limited treatment options. The rapid development of next-generation sequencing technology has brought the diagnosis and treatment of neoplastic diseases to the era of precision medicine.<span><sup>2</sup></span> It provided detailed RNA-seq information for the prognosis and prediction of different therapies and guided the crucial clinical decision-making processes throughout the treatment.<span><sup>3</sup></span> Here, we aim to develop prognosis-oriented molecular subtyping of RPLS and further provide novel treatment strategies for RPLS patients (Figure 1A). This work fundamentally differs from our previous reports.<span><sup>4</sup></span> It focuses on prognostic genes rather than differential genes, employing Weighted Gene Network Analysis and nonnegative matrix factorization (NMF) algorithms to achieve a more refined molecular classification of RPLS. By selecting and validating representative molecular biomarkers for each subtype, we have further streamlined the classification system for clinical application. Additionally, this classification system elucidates how the molecular biological characteristics of the different subtypes influence distinct clinical prognoses.</p><p>To construct prognosis-oriented RPLS molecular subtypes, we first identify the prognostic genes in our training cohort based on univariate cox regression (<i>N</i> = 80, Table 1; Tables S1 and S2). The regression analysis pipeline was conducted with the R package “survival” (Supporting Information Material and methods). A total of 3550 genes were associated with OS and DFS (<i>p </i>< .05; Figure 1B), and the top 10 genes of HR > 1 and HR < 1 were shown in Figure 1C. Functional annotation revealed these genes were enriched in the cell cycle, TGFβ-signalling pathway, angiopoietin, and cellular senescence (Figure 1D–F). We then functionally clustered 3550 prognostic genes by WGCNA (Figure S1) and selected the top 20 genes in each module for NMF grouping. Three RPLS subtypes were significantly distinguished (Figure 1G–H). Log-rank analysis showed that subtype 2 (S2) had the best prognostic outcomes (including OS, <i>p</i> < .0046; DFS, <i>p</i> < .0001) compared with subtype 1 (S1) and subtype 3 (S3), while S3 had the worst prognostic outcomes among them (Figure 2A,B). Functional annotation of characteristic genes showed that “Obesity”, “Overnutrition”, and “<i>PPAR</i> signaling pathway” were mainly enrichment terms of S2 (Figure S2).</p><p>Hallmark gene set of cancer well represents the specific biological processes and states of tumours. We previously revealed the differences in the functional annotation among subtypes. To verify them, hallmark gene sets were scored on patients of each subtype by ssGSEA. We found that metabolism-related pathways, including “adipogenesis” and “bile acid metabolism”, were most strongly associated with S2. This observation is consistent with recent studies that elucidate the role of bile acids in modulating the tumour immune microenvironment, as well as their involvement in lipogenesis, metabolism, and the regulation of tumour proliferation and apoptosis.<span><sup>5-7</sup></span> These findings underscore the critical role of bile acids in tumorigenesis and progression. Proliferation-related pathways, such as “mitotic spindle” and “G2M checkpoint” were the most important biological processes in S3, while immune-related pathways, such as “TNFα”, “IL2-STAT5” and “IFNα and IFNβ response” were mainly enriched in S1 (Figure 2C). Although activation of immune responses can significantly inhibit tumour progression, concomitant upregulation of PI3K-Akt-mTOR and KRAS signalling pathways reduces S1 prognosis.<span><sup>8</sup></span> We also evaluated the tumour microenvironment (TME, using the ESTIMATE algorithm) and clinical signatures (using one-way ANOVA) among three subtypes (Supplementary material and methods), the results showed that S3 had the lowest TME score and smallest tumour size (Figure 2D,E), but had the highest MDM2 expression, Ki67 index and FNCLCC score (Figure 2F,H), the most surgery times (Figure 2I), and the most significant pathological subtype ratio (DDLS/WDLS) among them (Figure 2J). These results demonstrated that the subtypes exhibited distinct biological features connecting the clinical, pathological, and prognostic signatures of RPLS.</p><p>For the NMF classification of RPLS patients, KLF6, ECM2, and LMNB2 were identified as representative biomarkers of S1, S2, and S3, respectively (Figure 2K and Figure S3). We then performed log-rank analysis according to the expression level of the three biomarkers, and the results showed that RPLS patients with high expressed KLF6 and ECM2 had better OS (KLF6: <i>p</i> = .034; ECM2: <i>p</i> = .035; Figure 2L,N) and DFS (KLF6: <i>p</i> = .0096; ECM2: <i>p</i> < .001; Figure 2M,O). However, Patients with high expressed LMNB2 had worse OS (<i>p</i> = .013, Figure 2P) and DFS (<i>p</i> < .001, Figure 2Q). KLF6 and ECM2 were important tumour suppressors in many tumours, they acted a beneficial role by inactivating p38/JNK/ERK signalling and increasing p21 in a p53-independent manner.<span><sup>9, 10</sup></span> LMNB2 is crucial in maintaining the integrity of the nuclear skeleton and participating in cell proliferation, ageing, and DNA damage repair.<span><sup>11</sup></span> It promotes the progression of these tumours by silencing p21, ki67, and caspase3, activating CDCA3, and regulating immune infiltrates.<span><sup>12-14</sup></span> These results suggest that the representative biomarkers are prognostic molecules in nature, which echoes our initial design idea of establishing prognosis-oriented molecular subtypes of RPLS.</p><p>Finally, we validated the representative biomarkers in the Retroperitoneal Sarcoma Registry (RESAR) cohort (<i>N</i> = 174, NCT03838718, Table 1). IHC staining was performed as previously described (Supporting Information Material and Methods) and the representative images with different degrees of expression are shown in Figure 3A. These classifications are derived from a comprehensive evaluation of biomarkers’ expression across all validation cohort samples, with the lowest one-third designated as low expression, the middle one-third as intermediate expression, and the highest one-third as high expression. We found that RPLS patients with higher <i>KLF6</i> and <i>ECM2</i> had better OS (Figure 3B,D) and DFS (Figure 3C,E) than those with lower expression, whereas patients with higher <i>LMNB2</i> had worse OS and DFS than patients with lower expression (Figure 3F,G). It is consistent with our previous findings in our training cohort. To further validate the three-gene-based molecular subtypes, we divided RPLS patients into three subgroups for prognosis analysis according to which biomarker (<i>KLF6</i>, <i>ECM2</i>, and <i>LMNB2</i>) showed the highest expression (Table S3). The <i>ECM2</i> subgroup had the best OS and DFS, whereas the <i>LMNB2</i> subgroup had the poorest OS and DFS (Figure 3H,I). Besides, the highest pathological subtype ratio (DDLS/WDLS), <i>Ki67</i> level, and most surgery times (Figure 3J–L) were observed in the <i>LMNB2</i> subgroup, in accordance with disease progression.</p><p>To sum up, we proposed three RPLS subtypes with IHC-verified biomarkers. The new classification of RPLS revealed distinct biological features and indicated various prognoses. It would be a preliminary but essential effort to bring RPLS treatment to the precision medicine era.</p><p>Conception/design: Li Min, Chenghua Luo; provision of study material or patients: Chenghua Luo, Mengmeng Xiao, Shixiang Ma, Xiaobing Chen; collection and/or assembly of data: Da Qin, Xiangji Li, Fanqin Bu, Yu Zhao; data analysis and interpretation: Xiangji Li, Da Qin, Fanqin Bu; manuscript writing: Mengmeng Xiao, Xiangji Li, Fanqin Bu, Li Min; final approval of manuscript: Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min.</p><p>The authors declare no conflict of interest.</p><p>This work was supported by grants from the Young Elite Scientists Sponsorship Program (2023QNRC001) and the National Natural Science Foundation of China (82073390). The study sponsors had no role in the design and preparation of this manuscript.</p><p>Specimens of RPLS patients were obtained from Peking University International Hospital. The experiments were undertaken with the understanding and written consent of each subject. The study protocol conformed to the standards set by the Declaration of Helsinki and was approved by the Ethics Committee of Peking University International Hospital, Peking University Health Science Center (WA2020RW29).</p><p>All authors have read and approved the manuscript and agree with submission to Clinical and Translational Medicine.</p>\",\"PeriodicalId\":10189,\"journal\":{\"name\":\"Clinical and Translational Medicine\",\"volume\":\"14 10\",\"pages\":\"\"},\"PeriodicalIF\":6.8000,\"publicationDate\":\"2024-10-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.70050\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70050\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70050","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Prognosis-oriented molecular subtypes of retroperitoneal liposarcoma
Dear Editor,
Retroperitoneal liposarcoma (RPLS) is an extremely rare malignant tumour.1 It is largely understudied with unknown risk factors and limited treatment options. The rapid development of next-generation sequencing technology has brought the diagnosis and treatment of neoplastic diseases to the era of precision medicine.2 It provided detailed RNA-seq information for the prognosis and prediction of different therapies and guided the crucial clinical decision-making processes throughout the treatment.3 Here, we aim to develop prognosis-oriented molecular subtyping of RPLS and further provide novel treatment strategies for RPLS patients (Figure 1A). This work fundamentally differs from our previous reports.4 It focuses on prognostic genes rather than differential genes, employing Weighted Gene Network Analysis and nonnegative matrix factorization (NMF) algorithms to achieve a more refined molecular classification of RPLS. By selecting and validating representative molecular biomarkers for each subtype, we have further streamlined the classification system for clinical application. Additionally, this classification system elucidates how the molecular biological characteristics of the different subtypes influence distinct clinical prognoses.
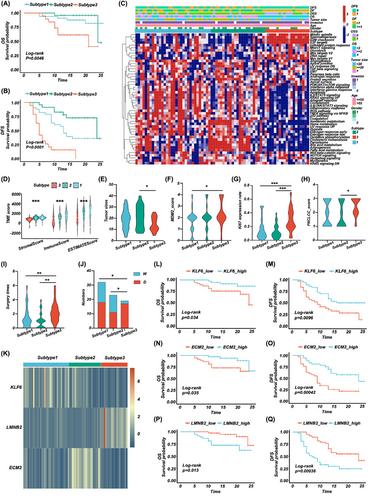
To construct prognosis-oriented RPLS molecular subtypes, we first identify the prognostic genes in our training cohort based on univariate cox regression (N = 80, Table 1; Tables S1 and S2). The regression analysis pipeline was conducted with the R package “survival” (Supporting Information Material and methods). A total of 3550 genes were associated with OS and DFS (p < .05; Figure 1B), and the top 10 genes of HR > 1 and HR < 1 were shown in Figure 1C. Functional annotation revealed these genes were enriched in the cell cycle, TGFβ-signalling pathway, angiopoietin, and cellular senescence (Figure 1D–F). We then functionally clustered 3550 prognostic genes by WGCNA (Figure S1) and selected the top 20 genes in each module for NMF grouping. Three RPLS subtypes were significantly distinguished (Figure 1G–H). Log-rank analysis showed that subtype 2 (S2) had the best prognostic outcomes (including OS, p < .0046; DFS, p < .0001) compared with subtype 1 (S1) and subtype 3 (S3), while S3 had the worst prognostic outcomes among them (Figure 2A,B). Functional annotation of characteristic genes showed that “Obesity”, “Overnutrition”, and “PPAR signaling pathway” were mainly enrichment terms of S2 (Figure S2).
Hallmark gene set of cancer well represents the specific biological processes and states of tumours. We previously revealed the differences in the functional annotation among subtypes. To verify them, hallmark gene sets were scored on patients of each subtype by ssGSEA. We found that metabolism-related pathways, including “adipogenesis” and “bile acid metabolism”, were most strongly associated with S2. This observation is consistent with recent studies that elucidate the role of bile acids in modulating the tumour immune microenvironment, as well as their involvement in lipogenesis, metabolism, and the regulation of tumour proliferation and apoptosis.5-7 These findings underscore the critical role of bile acids in tumorigenesis and progression. Proliferation-related pathways, such as “mitotic spindle” and “G2M checkpoint” were the most important biological processes in S3, while immune-related pathways, such as “TNFα”, “IL2-STAT5” and “IFNα and IFNβ response” were mainly enriched in S1 (Figure 2C). Although activation of immune responses can significantly inhibit tumour progression, concomitant upregulation of PI3K-Akt-mTOR and KRAS signalling pathways reduces S1 prognosis.8 We also evaluated the tumour microenvironment (TME, using the ESTIMATE algorithm) and clinical signatures (using one-way ANOVA) among three subtypes (Supplementary material and methods), the results showed that S3 had the lowest TME score and smallest tumour size (Figure 2D,E), but had the highest MDM2 expression, Ki67 index and FNCLCC score (Figure 2F,H), the most surgery times (Figure 2I), and the most significant pathological subtype ratio (DDLS/WDLS) among them (Figure 2J). These results demonstrated that the subtypes exhibited distinct biological features connecting the clinical, pathological, and prognostic signatures of RPLS.
For the NMF classification of RPLS patients, KLF6, ECM2, and LMNB2 were identified as representative biomarkers of S1, S2, and S3, respectively (Figure 2K and Figure S3). We then performed log-rank analysis according to the expression level of the three biomarkers, and the results showed that RPLS patients with high expressed KLF6 and ECM2 had better OS (KLF6: p = .034; ECM2: p = .035; Figure 2L,N) and DFS (KLF6: p = .0096; ECM2: p < .001; Figure 2M,O). However, Patients with high expressed LMNB2 had worse OS (p = .013, Figure 2P) and DFS (p < .001, Figure 2Q). KLF6 and ECM2 were important tumour suppressors in many tumours, they acted a beneficial role by inactivating p38/JNK/ERK signalling and increasing p21 in a p53-independent manner.9, 10 LMNB2 is crucial in maintaining the integrity of the nuclear skeleton and participating in cell proliferation, ageing, and DNA damage repair.11 It promotes the progression of these tumours by silencing p21, ki67, and caspase3, activating CDCA3, and regulating immune infiltrates.12-14 These results suggest that the representative biomarkers are prognostic molecules in nature, which echoes our initial design idea of establishing prognosis-oriented molecular subtypes of RPLS.
Finally, we validated the representative biomarkers in the Retroperitoneal Sarcoma Registry (RESAR) cohort (N = 174, NCT03838718, Table 1). IHC staining was performed as previously described (Supporting Information Material and Methods) and the representative images with different degrees of expression are shown in Figure 3A. These classifications are derived from a comprehensive evaluation of biomarkers’ expression across all validation cohort samples, with the lowest one-third designated as low expression, the middle one-third as intermediate expression, and the highest one-third as high expression. We found that RPLS patients with higher KLF6 and ECM2 had better OS (Figure 3B,D) and DFS (Figure 3C,E) than those with lower expression, whereas patients with higher LMNB2 had worse OS and DFS than patients with lower expression (Figure 3F,G). It is consistent with our previous findings in our training cohort. To further validate the three-gene-based molecular subtypes, we divided RPLS patients into three subgroups for prognosis analysis according to which biomarker (KLF6, ECM2, and LMNB2) showed the highest expression (Table S3). The ECM2 subgroup had the best OS and DFS, whereas the LMNB2 subgroup had the poorest OS and DFS (Figure 3H,I). Besides, the highest pathological subtype ratio (DDLS/WDLS), Ki67 level, and most surgery times (Figure 3J–L) were observed in the LMNB2 subgroup, in accordance with disease progression.
To sum up, we proposed three RPLS subtypes with IHC-verified biomarkers. The new classification of RPLS revealed distinct biological features and indicated various prognoses. It would be a preliminary but essential effort to bring RPLS treatment to the precision medicine era.
Conception/design: Li Min, Chenghua Luo; provision of study material or patients: Chenghua Luo, Mengmeng Xiao, Shixiang Ma, Xiaobing Chen; collection and/or assembly of data: Da Qin, Xiangji Li, Fanqin Bu, Yu Zhao; data analysis and interpretation: Xiangji Li, Da Qin, Fanqin Bu; manuscript writing: Mengmeng Xiao, Xiangji Li, Fanqin Bu, Li Min; final approval of manuscript: Mengmeng Xiao, Da Qin, Xiangji Li, Fanqin Bu, Shixiang Ma, Xiaobing Chen, Yu Zhao, Chenghua Luo, Li Min.
The authors declare no conflict of interest.
This work was supported by grants from the Young Elite Scientists Sponsorship Program (2023QNRC001) and the National Natural Science Foundation of China (82073390). The study sponsors had no role in the design and preparation of this manuscript.
Specimens of RPLS patients were obtained from Peking University International Hospital. The experiments were undertaken with the understanding and written consent of each subject. The study protocol conformed to the standards set by the Declaration of Helsinki and was approved by the Ethics Committee of Peking University International Hospital, Peking University Health Science Center (WA2020RW29).
All authors have read and approved the manuscript and agree with submission to Clinical and Translational Medicine.
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
