Clístenes C. de Carvalho, Idrys H. L. Guedes, Maria V. M. Dantas, Kariem El-Boghdadly
{"title":"由经验丰富的麻醉师进行气管插管的视频喉镜检查与直接喉镜检查:随机对照试验的荟萃分析和试验顺序分析。","authors":"Clístenes C. de Carvalho, Idrys H. L. Guedes, Maria V. M. Dantas, Kariem El-Boghdadly","doi":"10.1111/anae.16448","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":7742,"journal":{"name":"Anaesthesia","volume":"79 12","pages":"1371-1373"},"PeriodicalIF":7.4000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16448","citationCount":"0","resultStr":"{\"title\":\"Videolaryngoscopy vs. direct laryngoscopy for tracheal intubation by experienced anaesthetists: a meta-analysis and trial sequential analysis of randomised controlled trials\",\"authors\":\"Clístenes C. de Carvalho, Idrys H. L. Guedes, Maria V. M. Dantas, Kariem El-Boghdadly\",\"doi\":\"10.1111/anae.16448\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"\",\"PeriodicalId\":7742,\"journal\":{\"name\":\"Anaesthesia\",\"volume\":\"79 12\",\"pages\":\"1371-1373\"},\"PeriodicalIF\":7.4000,\"publicationDate\":\"2024-10-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/anae.16448\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anaesthesia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/ftr/10.1111/anae.16448\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/ftr/10.1111/anae.16448","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
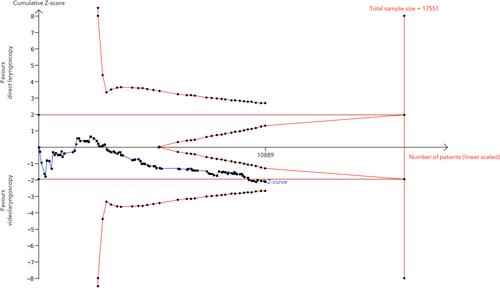
Videolaryngoscopy vs. direct laryngoscopy for tracheal intubation by experienced anaesthetists: a meta-analysis and trial sequential analysis of randomised controlled trials
期刊介绍:
The official journal of the Association of Anaesthetists is Anaesthesia. It is a comprehensive international publication that covers a wide range of topics. The journal focuses on general and regional anaesthesia, as well as intensive care and pain therapy. It includes original articles that have undergone peer review, covering all aspects of these fields, including research on equipment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
