Peter Kaiser, Gernot Schmidle, Simone Bode, Ulrike Seeher, Hanne-Rose Honis, Bernhard Moriggl, Elisabeth Pechriggl, Hannes Stofferin, Marko Konschake
{"title":"关于微创腕管松解术的腕管临床应用解剖学。","authors":"Peter Kaiser, Gernot Schmidle, Simone Bode, Ulrike Seeher, Hanne-Rose Honis, Bernhard Moriggl, Elisabeth Pechriggl, Hannes Stofferin, Marko Konschake","doi":"10.1007/s00402-024-05560-7","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Carpal tunnel release is a widely performed procedure. Despite a high success rate, iatrogenic neurovascular injuries can occur which lead to a painful and unsatisfying outcome. This study conducted a detailed examination of the anatomy of the carpal tunnel and the proximity of neurovascular structures that are particularly susceptible to injury, especially in the context of minimally invasive carpal tunnel release procedures.</p><h3>Patients and methods</h3><p>The anatomy of the carpal tunnel of 104 wrists of 52 body donors was examined. The precise anatomical location and the presence of variations were recorded for the median nerve, ulnar nerve, ulnar artery and Berrettini branch. The distance between the median nerve, the ulnar artery, the ulnar nerve, and the Berrettini branch was measured in a proximo-distal and radio-ulnar direction in relation to the distal ulnar end of the carpal tunnel.</p><h3>Results</h3><p>The authors identified four main dangerous anatomical situations. (1) A proximal separation of the Long-Finger/Ring-Finger branch of the median nerve together with a narrow safe-zone; (2) an ulnar take-off of the recurrent muscle branch of the median nerve with a close radio-ulnar distance to the distal ulnar end of carpal tunnel; (3) an ulnar arterial arch lying close to the transverse carpal ligament; and (4) a proximal Berrettini branch also lying close to the latter. All situations are illustrated by photographs. Additionally, the authors present a sonographic carpal tunnel assessment protocol in order to reduce the risk of injury of any neurovascular structure in the proximity of the carpal tunnel.</p><h3>Conclusion</h3><p>Certain patients may inherently face an increased risk of neurovascular injuries during minimally invasive carpal tunnel releases due to their anatomical variations. Four potentially risky scenarios were clearly illustrated. Consequently, one may consider conducting a preoperative ultrasound assessment of neurovascular structures at risk, when endoscopic or ultrasound-guided tunnel release are planned. In high-risk patients, open surgery should be preferred.</p><h3>Level of evidence</h3><p>II.</p></div>","PeriodicalId":8326,"journal":{"name":"Archives of Orthopaedic and Trauma Surgery","volume":"144 :","pages":"4753 - 4765"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11582268/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical-applied anatomy of the carpal tunnel regarding mini-invasive carpal tunnel release\",\"authors\":\"Peter Kaiser, Gernot Schmidle, Simone Bode, Ulrike Seeher, Hanne-Rose Honis, Bernhard Moriggl, Elisabeth Pechriggl, Hannes Stofferin, Marko Konschake\",\"doi\":\"10.1007/s00402-024-05560-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Carpal tunnel release is a widely performed procedure. Despite a high success rate, iatrogenic neurovascular injuries can occur which lead to a painful and unsatisfying outcome. This study conducted a detailed examination of the anatomy of the carpal tunnel and the proximity of neurovascular structures that are particularly susceptible to injury, especially in the context of minimally invasive carpal tunnel release procedures.</p><h3>Patients and methods</h3><p>The anatomy of the carpal tunnel of 104 wrists of 52 body donors was examined. The precise anatomical location and the presence of variations were recorded for the median nerve, ulnar nerve, ulnar artery and Berrettini branch. The distance between the median nerve, the ulnar artery, the ulnar nerve, and the Berrettini branch was measured in a proximo-distal and radio-ulnar direction in relation to the distal ulnar end of the carpal tunnel.</p><h3>Results</h3><p>The authors identified four main dangerous anatomical situations. (1) A proximal separation of the Long-Finger/Ring-Finger branch of the median nerve together with a narrow safe-zone; (2) an ulnar take-off of the recurrent muscle branch of the median nerve with a close radio-ulnar distance to the distal ulnar end of carpal tunnel; (3) an ulnar arterial arch lying close to the transverse carpal ligament; and (4) a proximal Berrettini branch also lying close to the latter. All situations are illustrated by photographs. Additionally, the authors present a sonographic carpal tunnel assessment protocol in order to reduce the risk of injury of any neurovascular structure in the proximity of the carpal tunnel.</p><h3>Conclusion</h3><p>Certain patients may inherently face an increased risk of neurovascular injuries during minimally invasive carpal tunnel releases due to their anatomical variations. Four potentially risky scenarios were clearly illustrated. Consequently, one may consider conducting a preoperative ultrasound assessment of neurovascular structures at risk, when endoscopic or ultrasound-guided tunnel release are planned. In high-risk patients, open surgery should be preferred.</p><h3>Level of evidence</h3><p>II.</p></div>\",\"PeriodicalId\":8326,\"journal\":{\"name\":\"Archives of Orthopaedic and Trauma Surgery\",\"volume\":\"144 :\",\"pages\":\"4753 - 4765\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-10-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11582268/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Orthopaedic and Trauma Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s00402-024-05560-7\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Orthopaedic and Trauma Surgery","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s00402-024-05560-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Clinical-applied anatomy of the carpal tunnel regarding mini-invasive carpal tunnel release
Background
Carpal tunnel release is a widely performed procedure. Despite a high success rate, iatrogenic neurovascular injuries can occur which lead to a painful and unsatisfying outcome. This study conducted a detailed examination of the anatomy of the carpal tunnel and the proximity of neurovascular structures that are particularly susceptible to injury, especially in the context of minimally invasive carpal tunnel release procedures.
Patients and methods
The anatomy of the carpal tunnel of 104 wrists of 52 body donors was examined. The precise anatomical location and the presence of variations were recorded for the median nerve, ulnar nerve, ulnar artery and Berrettini branch. The distance between the median nerve, the ulnar artery, the ulnar nerve, and the Berrettini branch was measured in a proximo-distal and radio-ulnar direction in relation to the distal ulnar end of the carpal tunnel.
Results
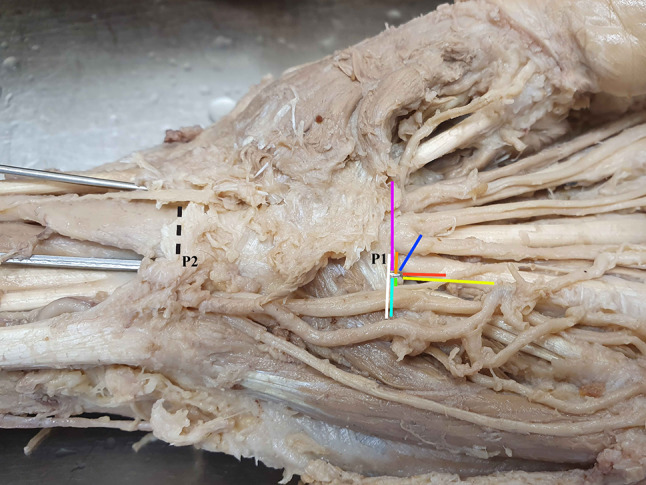
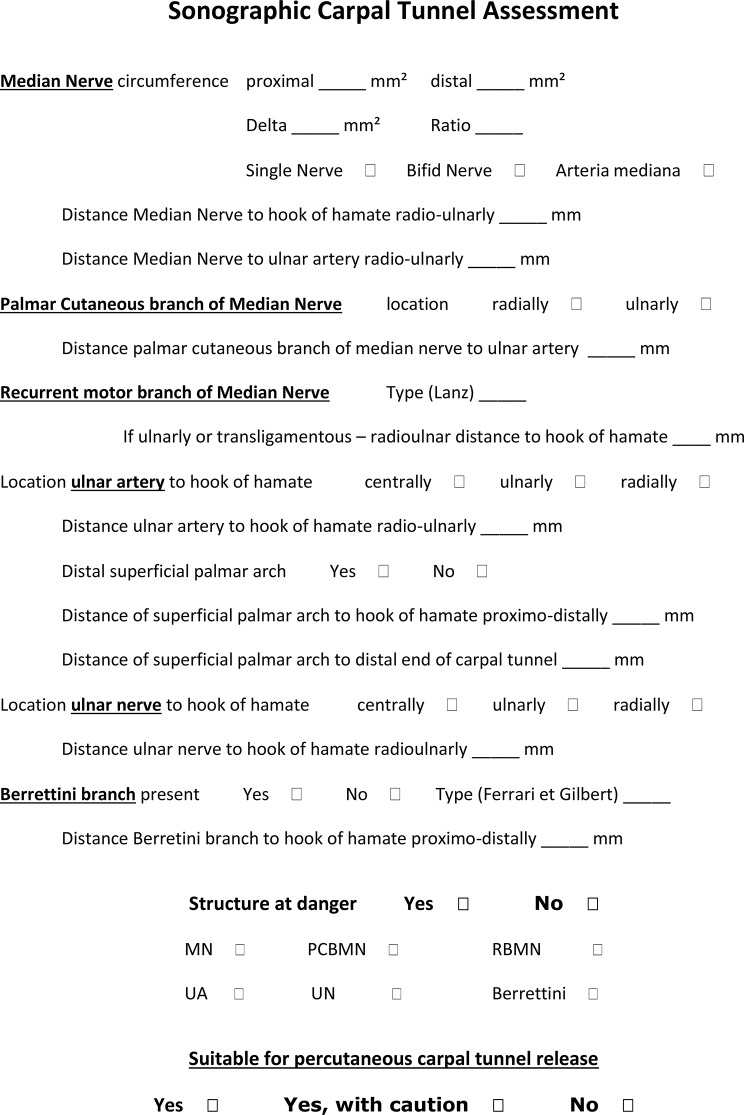
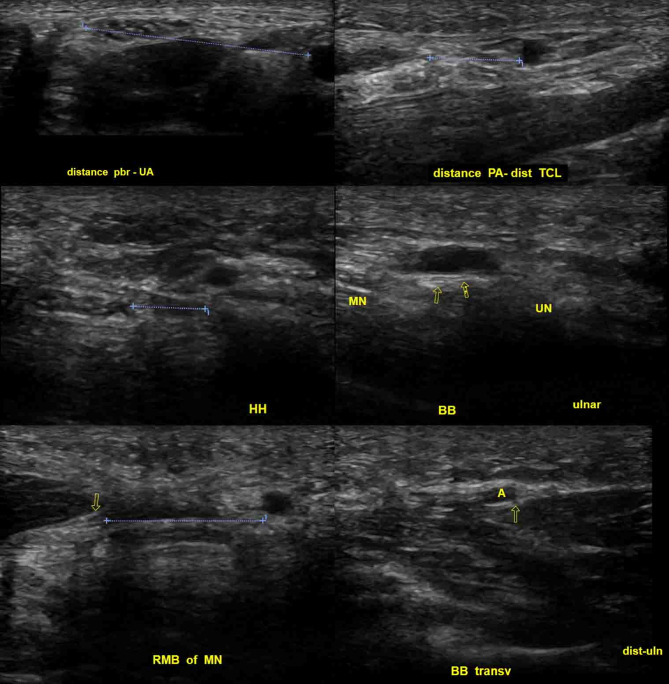
The authors identified four main dangerous anatomical situations. (1) A proximal separation of the Long-Finger/Ring-Finger branch of the median nerve together with a narrow safe-zone; (2) an ulnar take-off of the recurrent muscle branch of the median nerve with a close radio-ulnar distance to the distal ulnar end of carpal tunnel; (3) an ulnar arterial arch lying close to the transverse carpal ligament; and (4) a proximal Berrettini branch also lying close to the latter. All situations are illustrated by photographs. Additionally, the authors present a sonographic carpal tunnel assessment protocol in order to reduce the risk of injury of any neurovascular structure in the proximity of the carpal tunnel.
Conclusion
Certain patients may inherently face an increased risk of neurovascular injuries during minimally invasive carpal tunnel releases due to their anatomical variations. Four potentially risky scenarios were clearly illustrated. Consequently, one may consider conducting a preoperative ultrasound assessment of neurovascular structures at risk, when endoscopic or ultrasound-guided tunnel release are planned. In high-risk patients, open surgery should be preferred.
期刊介绍:
"Archives of Orthopaedic and Trauma Surgery" is a rich source of instruction and information for physicians in clinical practice and research in the extensive field of orthopaedics and traumatology. The journal publishes papers that deal with diseases and injuries of the musculoskeletal system from all fields and aspects of medicine. The journal is particularly interested in papers that satisfy the information needs of orthopaedic clinicians and practitioners. The journal places special emphasis on clinical relevance.
"Archives of Orthopaedic and Trauma Surgery" is the official journal of the German Speaking Arthroscopy Association (AGA).



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
