Beatrice Brett, Constantinos Savva, Bahar Mirshekar-Syahkal, Martyn Hill, Michael Douek, Ellen Copson, Ramsey Cutress
{"title":"早期乳腺癌新辅助内分泌治疗的手术效果:荟萃分析。","authors":"Beatrice Brett, Constantinos Savva, Bahar Mirshekar-Syahkal, Martyn Hill, Michael Douek, Ellen Copson, Ramsey Cutress","doi":"10.1093/bjsopen/zrae100","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant endocrine therapy presents an important downstaging option with lower toxicity than neoadjuvant chemotherapy in oestrogen receptor (ER)-positive early breast cancer. Meta-analysis of the effects of neoadjuvant endocrine therapy on surgical outcomes across randomized clinical trials (RCTs) and cohort studies has not previously been performed.</p><p><strong>Methods: </strong>A systematic review and meta-analysis was performed to evaluate the effect of neoadjuvant endocrine therapy on surgical outcomes (PROSPERO (international prospective register of systematic reviews, 2020)) compared with surgery followed by adjuvant endocrine therapy. PubMed and EMBASE were searched to identify RCT and cohort studies between 1946 and 27 March 2024. Two independent reviewers manually screened the identified records and extracted the data. Risk of bias was assessed using the Cochrane Collaboration tools and random-effects meta-analysis was done with ReviewManager.</p><p><strong>Results: </strong>The search identified 2390 articles eligible for screening. The review included 20 studies (12 cohort and 8 RCTs); 19 were included in the meta-analysis with a total of 6382 patients. Overall, neoadjuvant endocrine therapy was associated with a lower mastectomy rate compared with surgery first (risk ratio (RR) 0.53, 95% c.i. 0.44 to 0.64). Subgroup analysis showed similar improvement in the mastectomy rate in the neoadjuvant endocrine therapy group versus control group irrespective of study type (RCT: RR 0.58, 95% c.i. 0.50 to 0.66; cohorts: RR 0.48, 95% c.i. 0.33 to 0.70). There was no difference in the mastectomy rate by duration of neoadjuvant endocrine therapy (more than 4 months: RR 0.57, 95% c.i. 0.42 to 0.78; 4 months or less than 4 months: RR 0.52, 95% c.i. 0.43 to 0.64). Most of the studies were characterized by moderate-quality evidence with significant heterogeneity.</p><p><strong>Conclusion: </strong>Neoadjuvant endocrine therapy is associated with a reduction in mastectomy rate. Given the moderate methodological quality of previous studies, further RCTs are required.</p><p><strong>Registration id: </strong>CRD42020209257.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"8 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11488384/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical outcomes of neoadjuvant endocrine treatment in early breast cancer: meta-analysis.\",\"authors\":\"Beatrice Brett, Constantinos Savva, Bahar Mirshekar-Syahkal, Martyn Hill, Michael Douek, Ellen Copson, Ramsey Cutress\",\"doi\":\"10.1093/bjsopen/zrae100\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neoadjuvant endocrine therapy presents an important downstaging option with lower toxicity than neoadjuvant chemotherapy in oestrogen receptor (ER)-positive early breast cancer. Meta-analysis of the effects of neoadjuvant endocrine therapy on surgical outcomes across randomized clinical trials (RCTs) and cohort studies has not previously been performed.</p><p><strong>Methods: </strong>A systematic review and meta-analysis was performed to evaluate the effect of neoadjuvant endocrine therapy on surgical outcomes (PROSPERO (international prospective register of systematic reviews, 2020)) compared with surgery followed by adjuvant endocrine therapy. PubMed and EMBASE were searched to identify RCT and cohort studies between 1946 and 27 March 2024. Two independent reviewers manually screened the identified records and extracted the data. Risk of bias was assessed using the Cochrane Collaboration tools and random-effects meta-analysis was done with ReviewManager.</p><p><strong>Results: </strong>The search identified 2390 articles eligible for screening. The review included 20 studies (12 cohort and 8 RCTs); 19 were included in the meta-analysis with a total of 6382 patients. Overall, neoadjuvant endocrine therapy was associated with a lower mastectomy rate compared with surgery first (risk ratio (RR) 0.53, 95% c.i. 0.44 to 0.64). Subgroup analysis showed similar improvement in the mastectomy rate in the neoadjuvant endocrine therapy group versus control group irrespective of study type (RCT: RR 0.58, 95% c.i. 0.50 to 0.66; cohorts: RR 0.48, 95% c.i. 0.33 to 0.70). There was no difference in the mastectomy rate by duration of neoadjuvant endocrine therapy (more than 4 months: RR 0.57, 95% c.i. 0.42 to 0.78; 4 months or less than 4 months: RR 0.52, 95% c.i. 0.43 to 0.64). Most of the studies were characterized by moderate-quality evidence with significant heterogeneity.</p><p><strong>Conclusion: </strong>Neoadjuvant endocrine therapy is associated with a reduction in mastectomy rate. Given the moderate methodological quality of previous studies, further RCTs are required.</p><p><strong>Registration id: </strong>CRD42020209257.</p>\",\"PeriodicalId\":9028,\"journal\":{\"name\":\"BJS Open\",\"volume\":\"8 5\",\"pages\":\"\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2024-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11488384/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJS Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/bjsopen/zrae100\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae100","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Surgical outcomes of neoadjuvant endocrine treatment in early breast cancer: meta-analysis.
Background: Neoadjuvant endocrine therapy presents an important downstaging option with lower toxicity than neoadjuvant chemotherapy in oestrogen receptor (ER)-positive early breast cancer. Meta-analysis of the effects of neoadjuvant endocrine therapy on surgical outcomes across randomized clinical trials (RCTs) and cohort studies has not previously been performed.
Methods: A systematic review and meta-analysis was performed to evaluate the effect of neoadjuvant endocrine therapy on surgical outcomes (PROSPERO (international prospective register of systematic reviews, 2020)) compared with surgery followed by adjuvant endocrine therapy. PubMed and EMBASE were searched to identify RCT and cohort studies between 1946 and 27 March 2024. Two independent reviewers manually screened the identified records and extracted the data. Risk of bias was assessed using the Cochrane Collaboration tools and random-effects meta-analysis was done with ReviewManager.
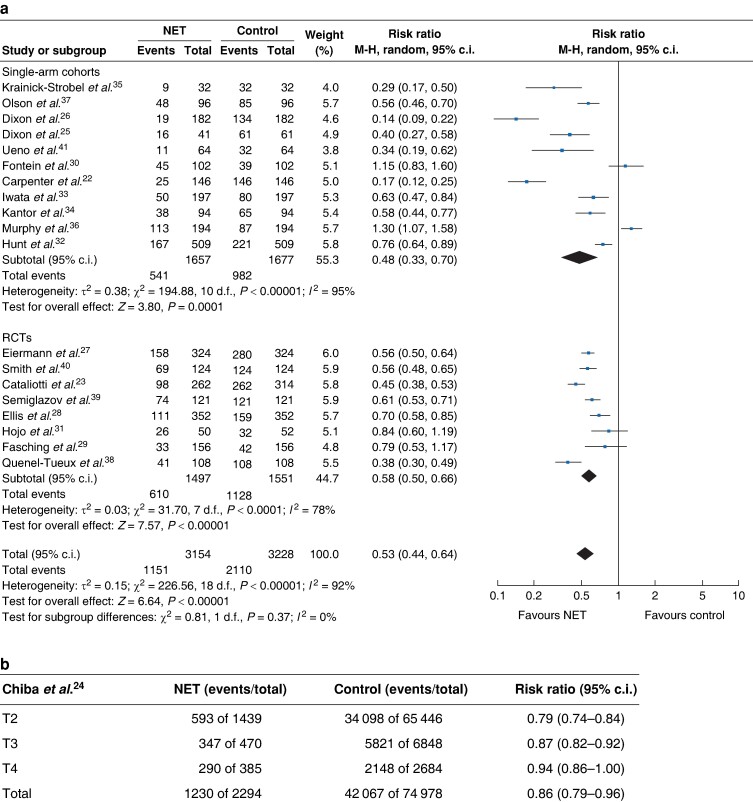
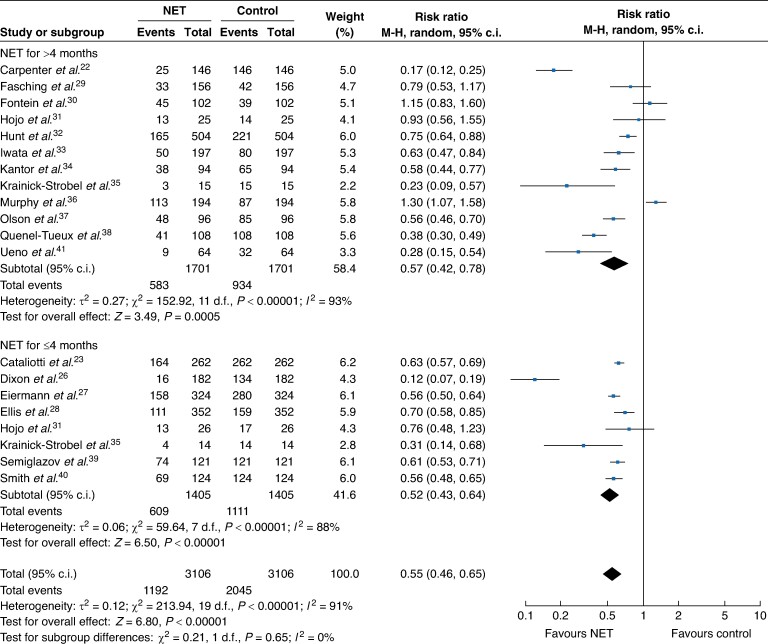
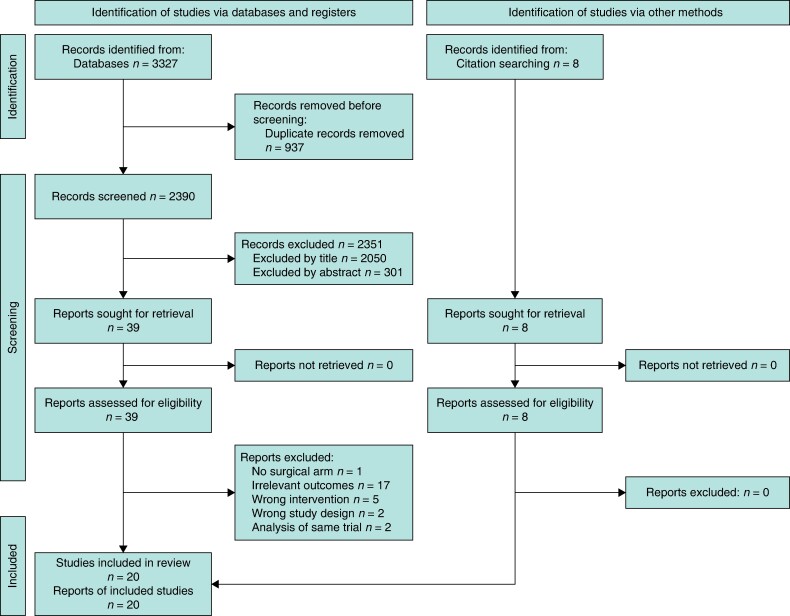
Results: The search identified 2390 articles eligible for screening. The review included 20 studies (12 cohort and 8 RCTs); 19 were included in the meta-analysis with a total of 6382 patients. Overall, neoadjuvant endocrine therapy was associated with a lower mastectomy rate compared with surgery first (risk ratio (RR) 0.53, 95% c.i. 0.44 to 0.64). Subgroup analysis showed similar improvement in the mastectomy rate in the neoadjuvant endocrine therapy group versus control group irrespective of study type (RCT: RR 0.58, 95% c.i. 0.50 to 0.66; cohorts: RR 0.48, 95% c.i. 0.33 to 0.70). There was no difference in the mastectomy rate by duration of neoadjuvant endocrine therapy (more than 4 months: RR 0.57, 95% c.i. 0.42 to 0.78; 4 months or less than 4 months: RR 0.52, 95% c.i. 0.43 to 0.64). Most of the studies were characterized by moderate-quality evidence with significant heterogeneity.
Conclusion: Neoadjuvant endocrine therapy is associated with a reduction in mastectomy rate. Given the moderate methodological quality of previous studies, further RCTs are required.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
