{"title":"肺癌伴非切除肺叶部分异常肺静脉连接:病例报告。","authors":"Yuuki Matsui, Koji Takami","doi":"10.1016/j.ijscr.2024.110454","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and importance: </strong>Partial anomalous pulmonary venous connection (PAPVC) is a relatively rare congenital vascular anomaly that complicates the surgical management of lung cancer and other lung lesions.</p><p><strong>Case presentation: </strong>A 74-year-old woman underwent computed tomography (CT) during an episode of chest trauma. Chest CT showed a 24-mm ground glass opacity in the right lower lobe and a PAPVC in the right upper lobe. She was diagnosed with suspected stage IA1 lung cancer with clinical T1miN0M0 and was scheduled for surgery. Preoperative catheterization revealed a pulmonary to systemic flow ratio (Qp/Qs) of 0.98. Surgical repair of PAPVC is indicated when the patient is symptomatic and has a Qp/Qs of 1.5 to 2.0 or more. The patient was scheduled for right lower lobectomy. Although worsening of postoperative right heart strain was considered, the Qp/Qs results indicated that surgical repair of the PAPVC was unnecessary. The intraoperative circulatory dynamics remained stable, and a right lower lobectomy was performed. Her postoperative course was uneventful. There was no evidence of right heart failure or recurrence of lung cancer at the last follow-up examination 6 and 12 months after surgery.</p><p><strong>Clinical discussion: </strong>If the PAPVC is in the non-resected lobe, preoperative assessment is really important, as major lung resection can increase shunt flow and cause right heart failure.</p><p><strong>Conclusion: </strong>We believe that careful interpretation of CT images of all pulmonary veins before major lung resection while considering PAPVC is important for safe perioperative management and adequate evaluation of cardiac dynamics when PAPVC is present.</p>","PeriodicalId":48113,"journal":{"name":"International Journal of Surgery Case Reports","volume":"124 ","pages":"110454"},"PeriodicalIF":0.7000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534182/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lung cancer associated with partial anomalous pulmonary venous connection in the non-resected lobe: A case report.\",\"authors\":\"Yuuki Matsui, Koji Takami\",\"doi\":\"10.1016/j.ijscr.2024.110454\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction and importance: </strong>Partial anomalous pulmonary venous connection (PAPVC) is a relatively rare congenital vascular anomaly that complicates the surgical management of lung cancer and other lung lesions.</p><p><strong>Case presentation: </strong>A 74-year-old woman underwent computed tomography (CT) during an episode of chest trauma. Chest CT showed a 24-mm ground glass opacity in the right lower lobe and a PAPVC in the right upper lobe. She was diagnosed with suspected stage IA1 lung cancer with clinical T1miN0M0 and was scheduled for surgery. Preoperative catheterization revealed a pulmonary to systemic flow ratio (Qp/Qs) of 0.98. Surgical repair of PAPVC is indicated when the patient is symptomatic and has a Qp/Qs of 1.5 to 2.0 or more. The patient was scheduled for right lower lobectomy. Although worsening of postoperative right heart strain was considered, the Qp/Qs results indicated that surgical repair of the PAPVC was unnecessary. The intraoperative circulatory dynamics remained stable, and a right lower lobectomy was performed. Her postoperative course was uneventful. There was no evidence of right heart failure or recurrence of lung cancer at the last follow-up examination 6 and 12 months after surgery.</p><p><strong>Clinical discussion: </strong>If the PAPVC is in the non-resected lobe, preoperative assessment is really important, as major lung resection can increase shunt flow and cause right heart failure.</p><p><strong>Conclusion: </strong>We believe that careful interpretation of CT images of all pulmonary veins before major lung resection while considering PAPVC is important for safe perioperative management and adequate evaluation of cardiac dynamics when PAPVC is present.</p>\",\"PeriodicalId\":48113,\"journal\":{\"name\":\"International Journal of Surgery Case Reports\",\"volume\":\"124 \",\"pages\":\"110454\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534182/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Surgery Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1016/j.ijscr.2024.110454\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Surgery Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.ijscr.2024.110454","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/12 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Lung cancer associated with partial anomalous pulmonary venous connection in the non-resected lobe: A case report.
Introduction and importance: Partial anomalous pulmonary venous connection (PAPVC) is a relatively rare congenital vascular anomaly that complicates the surgical management of lung cancer and other lung lesions.
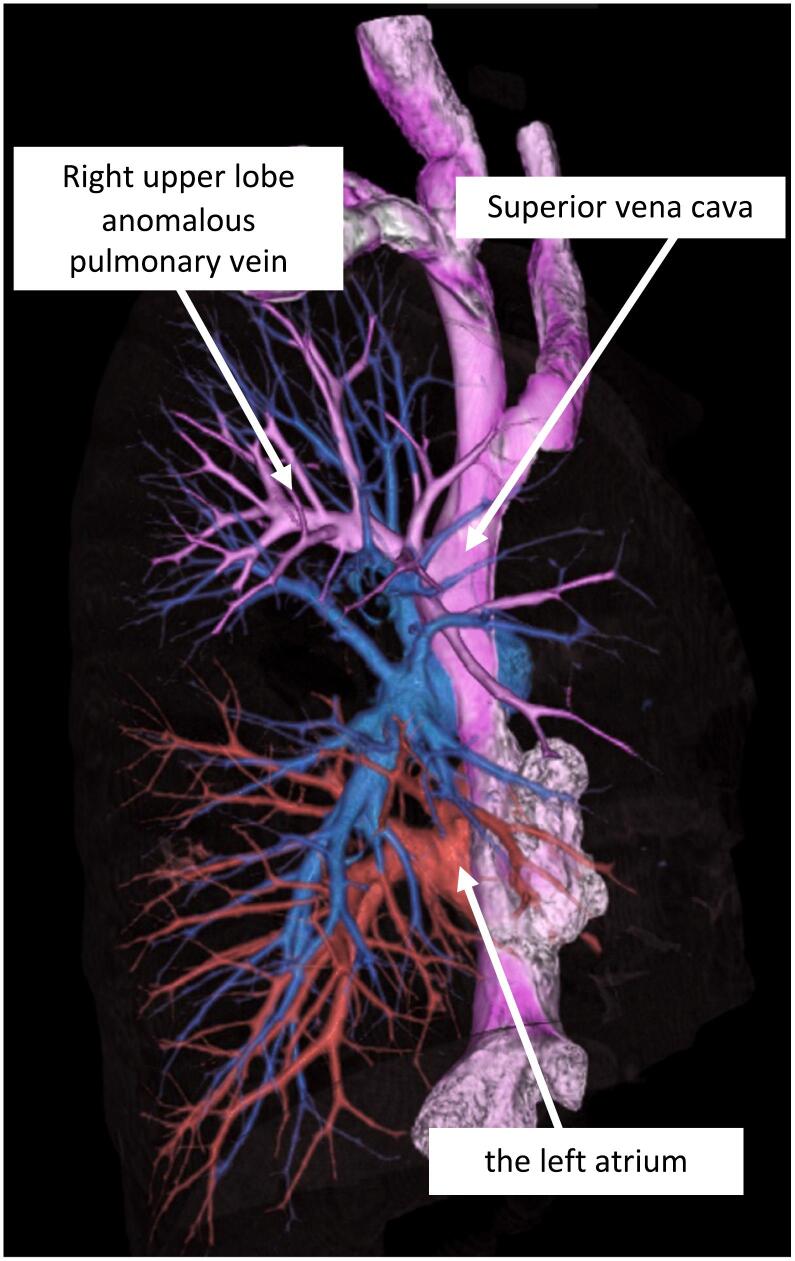
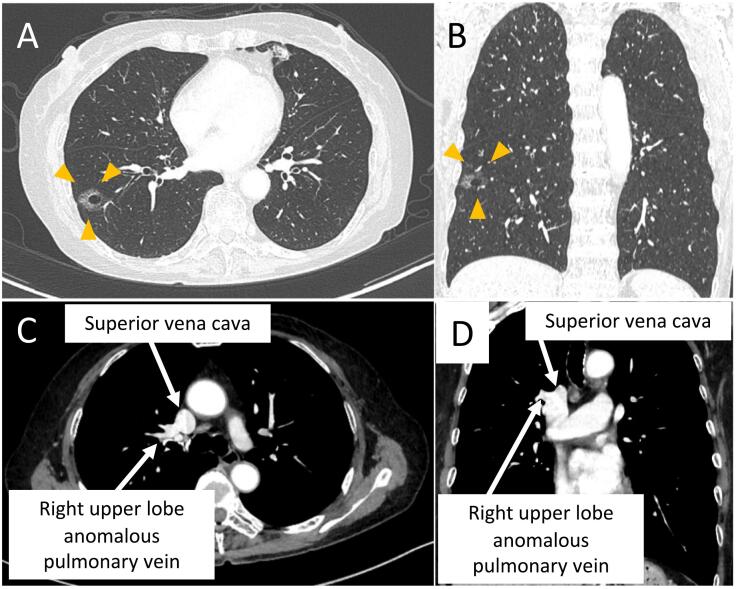
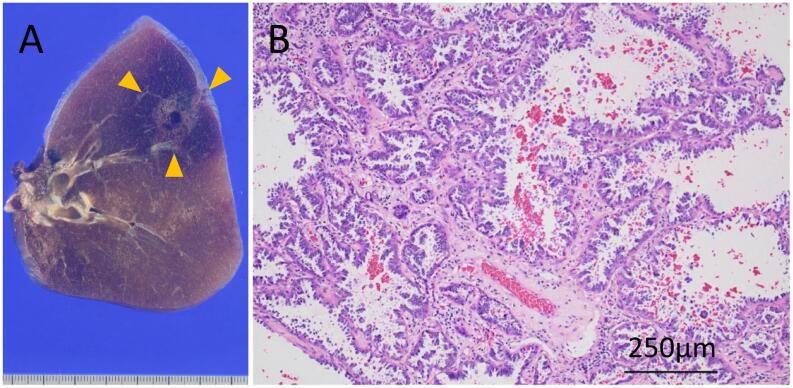
Case presentation: A 74-year-old woman underwent computed tomography (CT) during an episode of chest trauma. Chest CT showed a 24-mm ground glass opacity in the right lower lobe and a PAPVC in the right upper lobe. She was diagnosed with suspected stage IA1 lung cancer with clinical T1miN0M0 and was scheduled for surgery. Preoperative catheterization revealed a pulmonary to systemic flow ratio (Qp/Qs) of 0.98. Surgical repair of PAPVC is indicated when the patient is symptomatic and has a Qp/Qs of 1.5 to 2.0 or more. The patient was scheduled for right lower lobectomy. Although worsening of postoperative right heart strain was considered, the Qp/Qs results indicated that surgical repair of the PAPVC was unnecessary. The intraoperative circulatory dynamics remained stable, and a right lower lobectomy was performed. Her postoperative course was uneventful. There was no evidence of right heart failure or recurrence of lung cancer at the last follow-up examination 6 and 12 months after surgery.
Clinical discussion: If the PAPVC is in the non-resected lobe, preoperative assessment is really important, as major lung resection can increase shunt flow and cause right heart failure.
Conclusion: We believe that careful interpretation of CT images of all pulmonary veins before major lung resection while considering PAPVC is important for safe perioperative management and adequate evaluation of cardiac dynamics when PAPVC is present.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
