Fawaz Altuwaijri, Abdulaziz Alrabiah, Abdullah Alqarni, Alia Kamal Habash, Mohammad Alghofili, Omar Alotaibi, Mansour Altuwaijri
{"title":"高级心脏生命支持计划与成人高级生命支持计划的比较:基于模拟的试点研究。","authors":"Fawaz Altuwaijri, Abdulaziz Alrabiah, Abdullah Alqarni, Alia Kamal Habash, Mohammad Alghofili, Omar Alotaibi, Mansour Altuwaijri","doi":"10.1155/2024/6696879","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Cardiac arrest is a public health concern associated with unfavorable disease outcomes. Cardiopulmonary resuscitation (CPR) of optimal quality is widely acknowledged as an indispensable technique in restoring spontaneous circulation. In order to perform advanced cardiac life support (ACLS), chest compression must be paused twice: once to assess the rhythm and again to administer the shock. Australian advanced life support (ALS) recommends that the defibrillator needs to be precharged in order to administer the shock during a solitary interval in chest compressions. While performing chest compressions, precharging defibrillators can decrease hands-off time without posing a risk of injury. <b>Aim:</b> To compare chest compression fraction (CCF)-which is the cumulative time spent providing chest compressions divided by the total time taken for the entire resuscitation-by calculating the hands-off time duration in cardiac arrest between the Australian Resuscitation Council (ARC) and American Heart Association (AHA) protocols for CPR. <b>Methods:</b> A simulation-based pilot study was designed using a Laerdal Resusci Anne mannequin and a LIFEPACK 20 defibrillator. The study included six participants recruited from King Khalid University Hospital in Riyadh, Saudi Arabia, where three participants were certified ACLS providers and there were certified ALS providers. Participants were divided into two groups, ALS and ACLS, each following one protocol. For each scenario, a random job was assigned to each participant, regardless of their role as assistant, team leader, or performer of CPR. Each case's shockable and nonshockable rhythms were hidden from the team leader and the chest compressor. Ten trials of CPR were performed, each for four cycles with a total time of 8 min. The simulation was video recorded for hands-off time counting. Comparison between CCF (seconds) per cycle between the two protocols was performed using an independent sample <i>t</i>-test. A <i>p</i> value of 0.05 was used to measure statistical significance. <b>Results:</b> Comparing CCF in shockable rhythms between ARC and AHA protocols, it was observed that the CCF of ALS-ARC was significantly higher than ACLS-AHA in all cycles; the first cycle: <i>t</i> = 3.782, <i>p</i>=0.004; the second cycle: <i>t</i> = 3.380, <i>p</i>=0.007; the third cycle: <i>t</i> = 3.803, <i>p</i>=0.003; and the fourth cycle: <i>t</i> = 4.341, <i>p</i>=0.001. <b>Conclusion:</b> Precharging a defibrillator before a rhythm check during chest compression, in anticipation of a potentially shockable rhythm, reduces the time required for defibrillation and limits interruptions in chest compression during CPR. This practice effectively enhances the CCF. Enhancing the continuity of chest compressions can potentially improve survival rates in ARC.</p>","PeriodicalId":11528,"journal":{"name":"Emergency Medicine International","volume":"2024 ","pages":"6696879"},"PeriodicalIF":0.8000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511593/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison Between the Advanced Cardiac Life Support and Adult Advanced Life Support Protocols: A Simulation-Based Pilot Study.\",\"authors\":\"Fawaz Altuwaijri, Abdulaziz Alrabiah, Abdullah Alqarni, Alia Kamal Habash, Mohammad Alghofili, Omar Alotaibi, Mansour Altuwaijri\",\"doi\":\"10.1155/2024/6696879\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction:</b> Cardiac arrest is a public health concern associated with unfavorable disease outcomes. Cardiopulmonary resuscitation (CPR) of optimal quality is widely acknowledged as an indispensable technique in restoring spontaneous circulation. In order to perform advanced cardiac life support (ACLS), chest compression must be paused twice: once to assess the rhythm and again to administer the shock. Australian advanced life support (ALS) recommends that the defibrillator needs to be precharged in order to administer the shock during a solitary interval in chest compressions. While performing chest compressions, precharging defibrillators can decrease hands-off time without posing a risk of injury. <b>Aim:</b> To compare chest compression fraction (CCF)-which is the cumulative time spent providing chest compressions divided by the total time taken for the entire resuscitation-by calculating the hands-off time duration in cardiac arrest between the Australian Resuscitation Council (ARC) and American Heart Association (AHA) protocols for CPR. <b>Methods:</b> A simulation-based pilot study was designed using a Laerdal Resusci Anne mannequin and a LIFEPACK 20 defibrillator. The study included six participants recruited from King Khalid University Hospital in Riyadh, Saudi Arabia, where three participants were certified ACLS providers and there were certified ALS providers. Participants were divided into two groups, ALS and ACLS, each following one protocol. For each scenario, a random job was assigned to each participant, regardless of their role as assistant, team leader, or performer of CPR. Each case's shockable and nonshockable rhythms were hidden from the team leader and the chest compressor. Ten trials of CPR were performed, each for four cycles with a total time of 8 min. The simulation was video recorded for hands-off time counting. Comparison between CCF (seconds) per cycle between the two protocols was performed using an independent sample <i>t</i>-test. A <i>p</i> value of 0.05 was used to measure statistical significance. <b>Results:</b> Comparing CCF in shockable rhythms between ARC and AHA protocols, it was observed that the CCF of ALS-ARC was significantly higher than ACLS-AHA in all cycles; the first cycle: <i>t</i> = 3.782, <i>p</i>=0.004; the second cycle: <i>t</i> = 3.380, <i>p</i>=0.007; the third cycle: <i>t</i> = 3.803, <i>p</i>=0.003; and the fourth cycle: <i>t</i> = 4.341, <i>p</i>=0.001. <b>Conclusion:</b> Precharging a defibrillator before a rhythm check during chest compression, in anticipation of a potentially shockable rhythm, reduces the time required for defibrillation and limits interruptions in chest compression during CPR. This practice effectively enhances the CCF. Enhancing the continuity of chest compressions can potentially improve survival rates in ARC.</p>\",\"PeriodicalId\":11528,\"journal\":{\"name\":\"Emergency Medicine International\",\"volume\":\"2024 \",\"pages\":\"6696879\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2024-10-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511593/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency Medicine International\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2024/6696879\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine International","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2024/6696879","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
导言:心脏骤停是与不良疾病后果相关的公共卫生问题。最佳质量的心肺复苏术(CPR)被公认为是恢复自主循环不可或缺的技术。为了进行高级心脏生命支持(ACLS),胸外按压必须暂停两次:一次是为了评估心律,另一次是为了实施电击。澳大利亚高级生命支持(ALS)建议,需要对除颤器进行预充电,以便在胸外按压的短暂间歇中实施电击。在进行胸外心脏按压时,对除颤仪进行预充电可减少脱手时间,同时不会造成伤害风险。目的:通过计算澳大利亚复苏委员会(ARC)和美国心脏协会(AHA)心肺复苏协议中心脏骤停时的脱手时间,比较胸外按压分数(CCF),即胸外按压的累计时间除以整个复苏所需的总时间。方法:使用 Laerdal Resusci Anne 人体模型和 LIFEPACK 20 除颤器设计了一项基于模拟的试点研究。该研究包括从沙特阿拉伯利雅得国王哈立德大学医院招募的六名参与者,其中三名参与者是获得认证的 ACLS 提供者,另一名是获得认证的 ALS 提供者。参与者被分为 ALS 和 ACLS 两组,每组遵循一个方案。在每个场景中,随机为每位参与者分配一项工作,无论其角色是助理、组长还是心肺复苏术执行者。每个病例的可电击和不可电击节律都对组长和胸外按压器保密。进行了 10 次心肺复苏试验,每次 4 个周期,总时间为 8 分钟。模拟操作过程进行了录像,以便进行脱手时间计算。使用独立样本 t 检验比较两种方案每个循环的 CCF(秒)。统计显著性以 p 值 0.05 为标准。结果比较 ARC 和 AHA 方案在可电击节律中的 CCF,发现 ALS-ARC 在所有周期的 CCF 都明显高于 ACLS-AHA;第一个周期:t = 3.782,p=0.004;第二个周期:t = 3.380,p=0.007;第三个周期:t = 3.803,p=0.003;第四个周期:t = 4.341,p=0.001。结论在胸外按压过程中进行心律检查之前对除颤器进行预充电,以预测可能出现的可电击心律,可缩短除颤所需的时间,并限制心肺复苏过程中胸外按压的中断。这种做法可有效增强 CCF。加强胸外按压的连续性有可能提高 ARC 的存活率。
Comparison Between the Advanced Cardiac Life Support and Adult Advanced Life Support Protocols: A Simulation-Based Pilot Study.
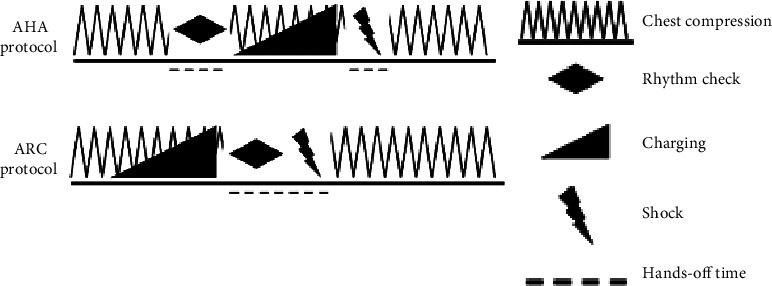
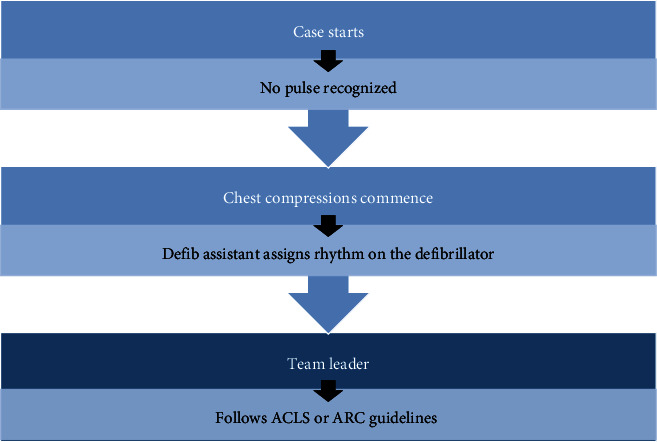
Introduction: Cardiac arrest is a public health concern associated with unfavorable disease outcomes. Cardiopulmonary resuscitation (CPR) of optimal quality is widely acknowledged as an indispensable technique in restoring spontaneous circulation. In order to perform advanced cardiac life support (ACLS), chest compression must be paused twice: once to assess the rhythm and again to administer the shock. Australian advanced life support (ALS) recommends that the defibrillator needs to be precharged in order to administer the shock during a solitary interval in chest compressions. While performing chest compressions, precharging defibrillators can decrease hands-off time without posing a risk of injury. Aim: To compare chest compression fraction (CCF)-which is the cumulative time spent providing chest compressions divided by the total time taken for the entire resuscitation-by calculating the hands-off time duration in cardiac arrest between the Australian Resuscitation Council (ARC) and American Heart Association (AHA) protocols for CPR. Methods: A simulation-based pilot study was designed using a Laerdal Resusci Anne mannequin and a LIFEPACK 20 defibrillator. The study included six participants recruited from King Khalid University Hospital in Riyadh, Saudi Arabia, where three participants were certified ACLS providers and there were certified ALS providers. Participants were divided into two groups, ALS and ACLS, each following one protocol. For each scenario, a random job was assigned to each participant, regardless of their role as assistant, team leader, or performer of CPR. Each case's shockable and nonshockable rhythms were hidden from the team leader and the chest compressor. Ten trials of CPR were performed, each for four cycles with a total time of 8 min. The simulation was video recorded for hands-off time counting. Comparison between CCF (seconds) per cycle between the two protocols was performed using an independent sample t-test. A p value of 0.05 was used to measure statistical significance. Results: Comparing CCF in shockable rhythms between ARC and AHA protocols, it was observed that the CCF of ALS-ARC was significantly higher than ACLS-AHA in all cycles; the first cycle: t = 3.782, p=0.004; the second cycle: t = 3.380, p=0.007; the third cycle: t = 3.803, p=0.003; and the fourth cycle: t = 4.341, p=0.001. Conclusion: Precharging a defibrillator before a rhythm check during chest compression, in anticipation of a potentially shockable rhythm, reduces the time required for defibrillation and limits interruptions in chest compression during CPR. This practice effectively enhances the CCF. Enhancing the continuity of chest compressions can potentially improve survival rates in ARC.
期刊介绍:
Emergency Medicine International is a peer-reviewed, Open Access journal that provides a forum for doctors, nurses, paramedics and ambulance staff. The journal publishes original research articles, review articles, and clinical studies related to prehospital care, disaster preparedness and response, acute medical and paediatric emergencies, critical care, sports medicine, wound care, and toxicology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
