Thomas Grischott, Tarun Mehra, Matthias R Meyer, Oliver Senn, Yael Rachamin
{"title":"在全国范围内禁止非急诊医疗期间的手术优先顺序:瑞士医院数据的准实验性回顾研究》。","authors":"Thomas Grischott, Tarun Mehra, Matthias R Meyer, Oliver Senn, Yael Rachamin","doi":"10.1177/11786329241293534","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>During the COVID-19 lockdown in spring 2020, Switzerland restricted non-urgent healthcare services to safeguard capacity. While prioritization of care was supposed to be driven by medical urgency, demographic factors or economic incentives might have influenced the hospitals' resource allocation decisions.</p><p><strong>Objectives: </strong>This study investigates potential determinants of procedure prioritization in hospitalized patients during the lockdown period.</p><p><strong>Design: </strong>Quasi-experimental retrospective study of hospital data in Switzerland.</p><p><strong>Methods: </strong>We analyzed 496 456 adult patients with known insurance status and a recorded procedure, admitted for cardiovascular, orthopedic/musculoskeletal or oncological reasons from January 2017 (3 years before the COVID-19 outbreak) to mid-April 2020 (in the first year of the COVID-19 pandemic), to obtain admission rate ratios (ARRs, \"lockdown\" admission rates divided by \"normal\" rates) from negative binomial regression analysis of fortnightly admissions for frequent procedure-diagnosis combinations. Quade and Wilcoxon signed-rank tests compared ARRs between sex×age, insurance and comorbidity strata.</p><p><strong>Results: </strong>Admission rates showed significant reductions for 29 of 53 procedure-diagnosis combinations. Reductions varied strongly by emergency, with largest decreases in orthopedic procedures for arthrosis (osteoarthritis) and non-arthritic joint disorders, and the smallest in cerebral imaging for stroke patients and surgical procedures for malignant neoplasms. The only difference in ARRs between strata was a stronger decrease in admission rates for cardiovascular combinations for patients with private versus basic health insurance.</p><p><strong>Conclusion: </strong>While medical procedures were affected to varying degrees by the ban on non-urgent healthcare during the COVID-19 lockdown, we found no robust evidence that factors other than medical urgency influenced healthcare prioritization.</p>","PeriodicalId":12876,"journal":{"name":"Health Services Insights","volume":"17 ","pages":"11786329241293534"},"PeriodicalIF":2.5000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11503697/pdf/","citationCount":"0","resultStr":"{\"title\":\"Procedure Prioritization During a Nationwide Ban on Non-Urgent Healthcare: A Quasi-Experimental Retrospective Study of Hospital Data in Switzerland.\",\"authors\":\"Thomas Grischott, Tarun Mehra, Matthias R Meyer, Oliver Senn, Yael Rachamin\",\"doi\":\"10.1177/11786329241293534\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>During the COVID-19 lockdown in spring 2020, Switzerland restricted non-urgent healthcare services to safeguard capacity. While prioritization of care was supposed to be driven by medical urgency, demographic factors or economic incentives might have influenced the hospitals' resource allocation decisions.</p><p><strong>Objectives: </strong>This study investigates potential determinants of procedure prioritization in hospitalized patients during the lockdown period.</p><p><strong>Design: </strong>Quasi-experimental retrospective study of hospital data in Switzerland.</p><p><strong>Methods: </strong>We analyzed 496 456 adult patients with known insurance status and a recorded procedure, admitted for cardiovascular, orthopedic/musculoskeletal or oncological reasons from January 2017 (3 years before the COVID-19 outbreak) to mid-April 2020 (in the first year of the COVID-19 pandemic), to obtain admission rate ratios (ARRs, \\\"lockdown\\\" admission rates divided by \\\"normal\\\" rates) from negative binomial regression analysis of fortnightly admissions for frequent procedure-diagnosis combinations. Quade and Wilcoxon signed-rank tests compared ARRs between sex×age, insurance and comorbidity strata.</p><p><strong>Results: </strong>Admission rates showed significant reductions for 29 of 53 procedure-diagnosis combinations. Reductions varied strongly by emergency, with largest decreases in orthopedic procedures for arthrosis (osteoarthritis) and non-arthritic joint disorders, and the smallest in cerebral imaging for stroke patients and surgical procedures for malignant neoplasms. The only difference in ARRs between strata was a stronger decrease in admission rates for cardiovascular combinations for patients with private versus basic health insurance.</p><p><strong>Conclusion: </strong>While medical procedures were affected to varying degrees by the ban on non-urgent healthcare during the COVID-19 lockdown, we found no robust evidence that factors other than medical urgency influenced healthcare prioritization.</p>\",\"PeriodicalId\":12876,\"journal\":{\"name\":\"Health Services Insights\",\"volume\":\"17 \",\"pages\":\"11786329241293534\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-10-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11503697/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Services Insights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11786329241293534\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11786329241293534","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Procedure Prioritization During a Nationwide Ban on Non-Urgent Healthcare: A Quasi-Experimental Retrospective Study of Hospital Data in Switzerland.
Background: During the COVID-19 lockdown in spring 2020, Switzerland restricted non-urgent healthcare services to safeguard capacity. While prioritization of care was supposed to be driven by medical urgency, demographic factors or economic incentives might have influenced the hospitals' resource allocation decisions.
Objectives: This study investigates potential determinants of procedure prioritization in hospitalized patients during the lockdown period.
Design: Quasi-experimental retrospective study of hospital data in Switzerland.
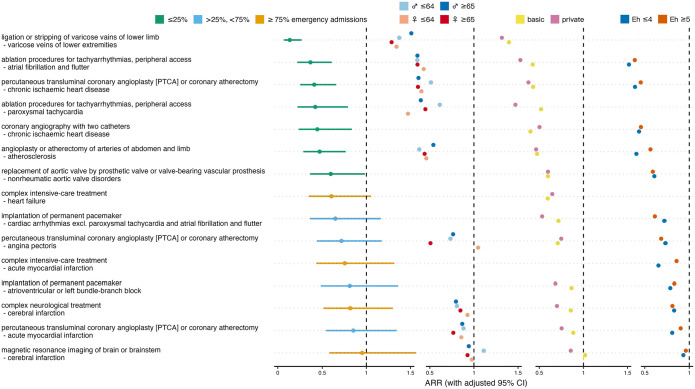
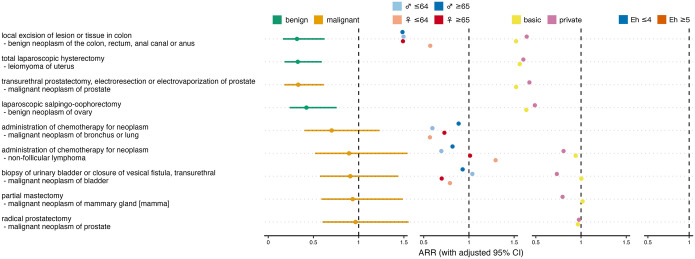
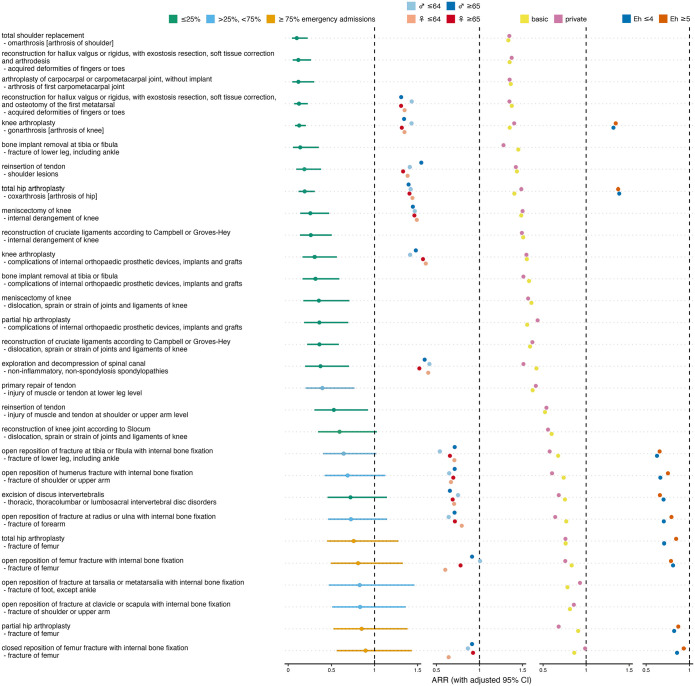
Methods: We analyzed 496 456 adult patients with known insurance status and a recorded procedure, admitted for cardiovascular, orthopedic/musculoskeletal or oncological reasons from January 2017 (3 years before the COVID-19 outbreak) to mid-April 2020 (in the first year of the COVID-19 pandemic), to obtain admission rate ratios (ARRs, "lockdown" admission rates divided by "normal" rates) from negative binomial regression analysis of fortnightly admissions for frequent procedure-diagnosis combinations. Quade and Wilcoxon signed-rank tests compared ARRs between sex×age, insurance and comorbidity strata.
Results: Admission rates showed significant reductions for 29 of 53 procedure-diagnosis combinations. Reductions varied strongly by emergency, with largest decreases in orthopedic procedures for arthrosis (osteoarthritis) and non-arthritic joint disorders, and the smallest in cerebral imaging for stroke patients and surgical procedures for malignant neoplasms. The only difference in ARRs between strata was a stronger decrease in admission rates for cardiovascular combinations for patients with private versus basic health insurance.
Conclusion: While medical procedures were affected to varying degrees by the ban on non-urgent healthcare during the COVID-19 lockdown, we found no robust evidence that factors other than medical urgency influenced healthcare prioritization.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
