{"title":"估算晚期肺癌患者不良事件的相关成本。","authors":"Chien-Yu Lin, Tzu-I Wu, Szu-Chun Yang","doi":"10.2147/CEOR.S489783","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to estimate the costs associated with adverse events (AEs) in advanced lung cancer patients treated with first-line therapies.</p><p><strong>Subjects and methods: </strong>All patients with advanced lung cancer diagnosed between 2011 and 2019 were identified from the Taiwan National Cancer Registry. First-line treatment was defined as a therapy that began within 30 days before and 90 days after the diagnosis. We defined a newly-developed AE as one established after first-line treatment had commenced, with the contingency that the patient had not been diagnosed with the AE within one year prior to the outset of therapy. One patient with a specific AE was matched on age, sex, and regimens with four patients without the AE. Payments incurred over the same period of time in the two groups were compared to estimate the AE-related costs.</p><p><strong>Results: </strong>A total of 27,376 patients receiving first-line targeted therapy, immunotherapy, or chemotherapy were identified. Clinical characteristics of 15,454 treatment episodes with a specific AE and 61,816 treatment episodes without the AE were well balanced. The costliest AEs of any severity were sepsis/septicemia, neuropathy, and acute kidney injury, with the respective average incremental costs of 10101, 9982, and 7839 USD. The costliest severe AEs requiring hospitalization were sepsis/septicemia, interstitial lung disease/pneumonitis, and neuropathy, with mean incremental costs of 22483, 10645, and 10120 USD, respectively.</p><p><strong>Conclusion: </strong>Costs associated with AEs in advanced lung cancer patients treated with first-line therapies were substantial. These estimates could be adopted for future cost-effectiveness analyses of new lung cancer treatments.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"16 ","pages":"761-769"},"PeriodicalIF":2.2000,"publicationDate":"2024-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11498143/pdf/","citationCount":"0","resultStr":"{\"title\":\"Estimating Costs Associated with Adverse Events in Patients with Advanced Lung Cancer.\",\"authors\":\"Chien-Yu Lin, Tzu-I Wu, Szu-Chun Yang\",\"doi\":\"10.2147/CEOR.S489783\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to estimate the costs associated with adverse events (AEs) in advanced lung cancer patients treated with first-line therapies.</p><p><strong>Subjects and methods: </strong>All patients with advanced lung cancer diagnosed between 2011 and 2019 were identified from the Taiwan National Cancer Registry. First-line treatment was defined as a therapy that began within 30 days before and 90 days after the diagnosis. We defined a newly-developed AE as one established after first-line treatment had commenced, with the contingency that the patient had not been diagnosed with the AE within one year prior to the outset of therapy. One patient with a specific AE was matched on age, sex, and regimens with four patients without the AE. Payments incurred over the same period of time in the two groups were compared to estimate the AE-related costs.</p><p><strong>Results: </strong>A total of 27,376 patients receiving first-line targeted therapy, immunotherapy, or chemotherapy were identified. Clinical characteristics of 15,454 treatment episodes with a specific AE and 61,816 treatment episodes without the AE were well balanced. The costliest AEs of any severity were sepsis/septicemia, neuropathy, and acute kidney injury, with the respective average incremental costs of 10101, 9982, and 7839 USD. The costliest severe AEs requiring hospitalization were sepsis/septicemia, interstitial lung disease/pneumonitis, and neuropathy, with mean incremental costs of 22483, 10645, and 10120 USD, respectively.</p><p><strong>Conclusion: </strong>Costs associated with AEs in advanced lung cancer patients treated with first-line therapies were substantial. These estimates could be adopted for future cost-effectiveness analyses of new lung cancer treatments.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"16 \",\"pages\":\"761-769\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-10-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11498143/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S489783\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S489783","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Estimating Costs Associated with Adverse Events in Patients with Advanced Lung Cancer.
Purpose: This study aimed to estimate the costs associated with adverse events (AEs) in advanced lung cancer patients treated with first-line therapies.
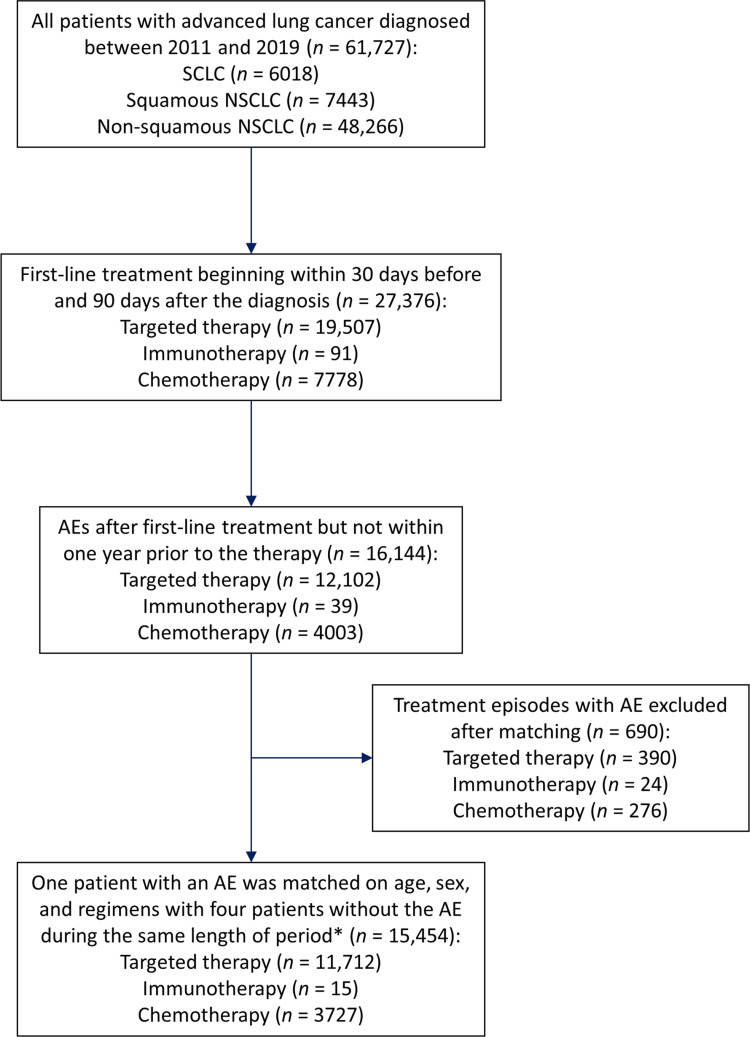
Subjects and methods: All patients with advanced lung cancer diagnosed between 2011 and 2019 were identified from the Taiwan National Cancer Registry. First-line treatment was defined as a therapy that began within 30 days before and 90 days after the diagnosis. We defined a newly-developed AE as one established after first-line treatment had commenced, with the contingency that the patient had not been diagnosed with the AE within one year prior to the outset of therapy. One patient with a specific AE was matched on age, sex, and regimens with four patients without the AE. Payments incurred over the same period of time in the two groups were compared to estimate the AE-related costs.
Results: A total of 27,376 patients receiving first-line targeted therapy, immunotherapy, or chemotherapy were identified. Clinical characteristics of 15,454 treatment episodes with a specific AE and 61,816 treatment episodes without the AE were well balanced. The costliest AEs of any severity were sepsis/septicemia, neuropathy, and acute kidney injury, with the respective average incremental costs of 10101, 9982, and 7839 USD. The costliest severe AEs requiring hospitalization were sepsis/septicemia, interstitial lung disease/pneumonitis, and neuropathy, with mean incremental costs of 22483, 10645, and 10120 USD, respectively.
Conclusion: Costs associated with AEs in advanced lung cancer patients treated with first-line therapies were substantial. These estimates could be adopted for future cost-effectiveness analyses of new lung cancer treatments.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
