{"title":"迷走神经刺激:通过减少细胞因子(白细胞介素-6)、减弱 SASP、增强肿瘤免疫力来治疗胶质母细胞瘤和实体瘤的新概念","authors":"Steven Brem","doi":"10.1016/j.bbih.2024.100859","DOIUrl":null,"url":null,"abstract":"<div><div>Immuno-oncology, specifically immune checkpoint inhibitors (ICIs), has revolutionized cancer care with dramatic, long-term responses and increased survival, including patients with metastatic cancer to the brain. Glioblastomas, and other primary brain tumors, are refractory to ICIs as monotherapy or in combination with standard therapy. The tumor microenvironment (TME) poses multiple biological hurdles: blood-brain barrier, immune suppression, heterogeneity, and tumor infiltration. Genomic analysis of the senescence-associated secretory phenotype (SASP) and preclinical models of glioma suggest that an exciting approach would entail reprogramming of the glioma microenvironment, attenuating the pro-inflammatory, pro-tumorigenic cytokines of the SASP, especially interleukin-6 (IL-6). A testable hypothesis now proposed is to modulate the immune system by harnessing the body's ‘inflammatory reflex’ to reduce cytokines. Vagus nerve stimulation can activate T cell immunity by the cholinergic, α7nicotinic acetylcholine receptor agonist (α7nAchR), and suppress IL-6 systemically, as well as other pro-inflammatory cytokines of the SASP, interleukin -1β (IL-1β) and tumor necrosis factor-alpha (TNF-α). The hypothesis predicts that electrical activation of the vagus nerve, with cytokine reduction, in combination with ICIs, would convert an immune resistant (“cold”) tumor to an immune responsive (“hot”) tumor, and halt glioma progression. The hypothesis also envisions cancer as an immune “dysautonomia” whereby a therapeutic intervention, vagus nerve stimulation (VNS), resets the systemic and local cytokine levels. A prospective, randomized, phase II clinical trial, to confirm the hypothesis, is a logical, exigent, next step. Cytokine reduction by VNS could also be useful for other forms of human cancer, e.g., breast, colorectal, head and neck, lung, melanoma, ovarian, pancreatic, and prostate cancer, as the emerging field of “cancer neuroscience” shows a role for neural regulation of multiple tumor types. Because IL-6, and companion pro-inflammatory cytokines, participate in the initiation, progression, spread and recurrence of cancer, minimally invasive VNS could be employed to suppress glioma or cancer progression, while also mitigating depression and/or seizures, thereby enhancing quality of life. The current hypothesis reimagines glioma pathophysiology as a dysautonomia with the therapeutic objective to reset the autonomic nervous system and form an immune responsive state to halt tumor progression and prevent recurrence. VNS, as a novel method to control cancer, can be administered with ICIs, standard therapy, or in clinical trials, combined with emerging immunotherapy: dendritic cell, mRNA, or chimeric antigen receptor (CAR) T cell vaccines.</div></div>","PeriodicalId":72454,"journal":{"name":"Brain, behavior, & immunity - health","volume":"42 ","pages":"Article 100859"},"PeriodicalIF":3.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Vagus nerve stimulation: Novel concept for the treatment of glioblastoma and solid cancers by cytokine (interleukin-6) reduction, attenuating the SASP, enhancing tumor immunity\",\"authors\":\"Steven Brem\",\"doi\":\"10.1016/j.bbih.2024.100859\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><div>Immuno-oncology, specifically immune checkpoint inhibitors (ICIs), has revolutionized cancer care with dramatic, long-term responses and increased survival, including patients with metastatic cancer to the brain. Glioblastomas, and other primary brain tumors, are refractory to ICIs as monotherapy or in combination with standard therapy. The tumor microenvironment (TME) poses multiple biological hurdles: blood-brain barrier, immune suppression, heterogeneity, and tumor infiltration. Genomic analysis of the senescence-associated secretory phenotype (SASP) and preclinical models of glioma suggest that an exciting approach would entail reprogramming of the glioma microenvironment, attenuating the pro-inflammatory, pro-tumorigenic cytokines of the SASP, especially interleukin-6 (IL-6). A testable hypothesis now proposed is to modulate the immune system by harnessing the body's ‘inflammatory reflex’ to reduce cytokines. Vagus nerve stimulation can activate T cell immunity by the cholinergic, α7nicotinic acetylcholine receptor agonist (α7nAchR), and suppress IL-6 systemically, as well as other pro-inflammatory cytokines of the SASP, interleukin -1β (IL-1β) and tumor necrosis factor-alpha (TNF-α). The hypothesis predicts that electrical activation of the vagus nerve, with cytokine reduction, in combination with ICIs, would convert an immune resistant (“cold”) tumor to an immune responsive (“hot”) tumor, and halt glioma progression. The hypothesis also envisions cancer as an immune “dysautonomia” whereby a therapeutic intervention, vagus nerve stimulation (VNS), resets the systemic and local cytokine levels. A prospective, randomized, phase II clinical trial, to confirm the hypothesis, is a logical, exigent, next step. Cytokine reduction by VNS could also be useful for other forms of human cancer, e.g., breast, colorectal, head and neck, lung, melanoma, ovarian, pancreatic, and prostate cancer, as the emerging field of “cancer neuroscience” shows a role for neural regulation of multiple tumor types. Because IL-6, and companion pro-inflammatory cytokines, participate in the initiation, progression, spread and recurrence of cancer, minimally invasive VNS could be employed to suppress glioma or cancer progression, while also mitigating depression and/or seizures, thereby enhancing quality of life. The current hypothesis reimagines glioma pathophysiology as a dysautonomia with the therapeutic objective to reset the autonomic nervous system and form an immune responsive state to halt tumor progression and prevent recurrence. VNS, as a novel method to control cancer, can be administered with ICIs, standard therapy, or in clinical trials, combined with emerging immunotherapy: dendritic cell, mRNA, or chimeric antigen receptor (CAR) T cell vaccines.</div></div>\",\"PeriodicalId\":72454,\"journal\":{\"name\":\"Brain, behavior, & immunity - health\",\"volume\":\"42 \",\"pages\":\"Article 100859\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brain, behavior, & immunity - health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666354624001376\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain, behavior, & immunity - health","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666354624001376","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Vagus nerve stimulation: Novel concept for the treatment of glioblastoma and solid cancers by cytokine (interleukin-6) reduction, attenuating the SASP, enhancing tumor immunity
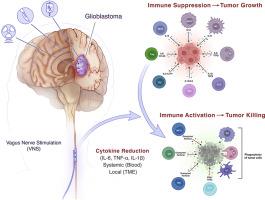
Immuno-oncology, specifically immune checkpoint inhibitors (ICIs), has revolutionized cancer care with dramatic, long-term responses and increased survival, including patients with metastatic cancer to the brain. Glioblastomas, and other primary brain tumors, are refractory to ICIs as monotherapy or in combination with standard therapy. The tumor microenvironment (TME) poses multiple biological hurdles: blood-brain barrier, immune suppression, heterogeneity, and tumor infiltration. Genomic analysis of the senescence-associated secretory phenotype (SASP) and preclinical models of glioma suggest that an exciting approach would entail reprogramming of the glioma microenvironment, attenuating the pro-inflammatory, pro-tumorigenic cytokines of the SASP, especially interleukin-6 (IL-6). A testable hypothesis now proposed is to modulate the immune system by harnessing the body's ‘inflammatory reflex’ to reduce cytokines. Vagus nerve stimulation can activate T cell immunity by the cholinergic, α7nicotinic acetylcholine receptor agonist (α7nAchR), and suppress IL-6 systemically, as well as other pro-inflammatory cytokines of the SASP, interleukin -1β (IL-1β) and tumor necrosis factor-alpha (TNF-α). The hypothesis predicts that electrical activation of the vagus nerve, with cytokine reduction, in combination with ICIs, would convert an immune resistant (“cold”) tumor to an immune responsive (“hot”) tumor, and halt glioma progression. The hypothesis also envisions cancer as an immune “dysautonomia” whereby a therapeutic intervention, vagus nerve stimulation (VNS), resets the systemic and local cytokine levels. A prospective, randomized, phase II clinical trial, to confirm the hypothesis, is a logical, exigent, next step. Cytokine reduction by VNS could also be useful for other forms of human cancer, e.g., breast, colorectal, head and neck, lung, melanoma, ovarian, pancreatic, and prostate cancer, as the emerging field of “cancer neuroscience” shows a role for neural regulation of multiple tumor types. Because IL-6, and companion pro-inflammatory cytokines, participate in the initiation, progression, spread and recurrence of cancer, minimally invasive VNS could be employed to suppress glioma or cancer progression, while also mitigating depression and/or seizures, thereby enhancing quality of life. The current hypothesis reimagines glioma pathophysiology as a dysautonomia with the therapeutic objective to reset the autonomic nervous system and form an immune responsive state to halt tumor progression and prevent recurrence. VNS, as a novel method to control cancer, can be administered with ICIs, standard therapy, or in clinical trials, combined with emerging immunotherapy: dendritic cell, mRNA, or chimeric antigen receptor (CAR) T cell vaccines.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
