Sandar Aye, Oskar Frisell, Henrik Zetterberg, Tobias Borgh Skillbäck, Silke Kern, Maria Eriksdotter, Emil Aho, Xin Xia, Bengt Winblad, Anders Wimo, Linus Jönsson
{"title":"瑞典阿尔茨海默病严重程度与护理成本的关系:基于国家登记的队列研究》。","authors":"Sandar Aye, Oskar Frisell, Henrik Zetterberg, Tobias Borgh Skillbäck, Silke Kern, Maria Eriksdotter, Emil Aho, Xin Xia, Bengt Winblad, Anders Wimo, Linus Jönsson","doi":"10.1007/s40273-024-01443-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The advancement of diagnostic and therapeutic interventions in early Alzheimer's disease (AD) has demanded the economic evaluation of such interventions. Resource utilization and cost estimates in early AD and, more specifically, the amyloid-positive population are still lacking. We aimed to provide cost estimates in AD in relation to disease severity and compare these with the control population. We also aimed to provide cost estimates for a subset of the AD population with both clinical diagnosis and amyloid-positive confirmation.</p><p><strong>Materials and methods: </strong>This was a retrospective longitudinal analysis of resource utilization using data from national registries. A cohort from the national Swedish registry for cognitive/dementia disorders (SveDem) includes all clinically diagnosed AD between 2013 and 2020. The study population included 31,951 people with AD and 63,902 age- and sex-matched controls (1:2). The population was followed until death, the end of December 2020, or 2 years from the last clinic visit. Direct medical and social costs were estimated from other national registries. Direct medical costs include costs for medications and inpatient and outpatient clinical visits. Direct social costs include costs for institutionalization, home care, short-term care, support for daytime activities, and housing support. Mean annual costs and 95% confidence intervals were obtained by bootstrapping, presented in 2021 Swedish Krona (SEK) (1 SEK = 0.117 USD, 1 SEK = 0.0985 EUR in 2021), and disaggregated by AD severity, cost component, sex, age group, and care setting.</p><p><strong>Results: </strong>Mean annual costs for individuals with clinically diagnosed AD were SEK 99,906, SEK 290,972, SEK 479,524, and SEK 795,617 in mild cognitive impairment (MCI), mild, moderate, and severe AD. The mean annual costs for the population with both clinical diagnosis and amyloid-positive AD confirmation (N = 5610) were SEK 57,625, SEK 179,153, SEK 333,095, and SEK 668,073 in MCI, mild, moderate, and severe AD, respectively. The mean annual costs were higher in institutionalized than non-institutionalized patients, females than males, and older than younger age groups. Inpatient and drug costs were similar in all AD severity stages, but outpatient costs decreased with AD severity. Costs for institutionalization, home care, support for daytime activities, and short-term care increased with AD severity, whereas the cost of housing support decreased with AD severity.</p><p><strong>Conclusions: </strong>This is the first study estimating annual costs in people with AD from MCI to severe AD, including those for the amyloid-positive population. The study provides cost estimates by AD severity, cost components, care settings, sex, and age groups, allowing health economic modelers to apply the costs based on different model structures and populations.</p>","PeriodicalId":19807,"journal":{"name":"PharmacoEconomics","volume":" ","pages":"153-169"},"PeriodicalIF":4.6000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11782292/pdf/","citationCount":"0","resultStr":"{\"title\":\"Costs of Care in Relation to Alzheimer's Disease Severity in Sweden: A National Registry-Based Cohort Study.\",\"authors\":\"Sandar Aye, Oskar Frisell, Henrik Zetterberg, Tobias Borgh Skillbäck, Silke Kern, Maria Eriksdotter, Emil Aho, Xin Xia, Bengt Winblad, Anders Wimo, Linus Jönsson\",\"doi\":\"10.1007/s40273-024-01443-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The advancement of diagnostic and therapeutic interventions in early Alzheimer's disease (AD) has demanded the economic evaluation of such interventions. Resource utilization and cost estimates in early AD and, more specifically, the amyloid-positive population are still lacking. We aimed to provide cost estimates in AD in relation to disease severity and compare these with the control population. We also aimed to provide cost estimates for a subset of the AD population with both clinical diagnosis and amyloid-positive confirmation.</p><p><strong>Materials and methods: </strong>This was a retrospective longitudinal analysis of resource utilization using data from national registries. A cohort from the national Swedish registry for cognitive/dementia disorders (SveDem) includes all clinically diagnosed AD between 2013 and 2020. The study population included 31,951 people with AD and 63,902 age- and sex-matched controls (1:2). The population was followed until death, the end of December 2020, or 2 years from the last clinic visit. Direct medical and social costs were estimated from other national registries. Direct medical costs include costs for medications and inpatient and outpatient clinical visits. Direct social costs include costs for institutionalization, home care, short-term care, support for daytime activities, and housing support. Mean annual costs and 95% confidence intervals were obtained by bootstrapping, presented in 2021 Swedish Krona (SEK) (1 SEK = 0.117 USD, 1 SEK = 0.0985 EUR in 2021), and disaggregated by AD severity, cost component, sex, age group, and care setting.</p><p><strong>Results: </strong>Mean annual costs for individuals with clinically diagnosed AD were SEK 99,906, SEK 290,972, SEK 479,524, and SEK 795,617 in mild cognitive impairment (MCI), mild, moderate, and severe AD. The mean annual costs for the population with both clinical diagnosis and amyloid-positive AD confirmation (N = 5610) were SEK 57,625, SEK 179,153, SEK 333,095, and SEK 668,073 in MCI, mild, moderate, and severe AD, respectively. The mean annual costs were higher in institutionalized than non-institutionalized patients, females than males, and older than younger age groups. Inpatient and drug costs were similar in all AD severity stages, but outpatient costs decreased with AD severity. Costs for institutionalization, home care, support for daytime activities, and short-term care increased with AD severity, whereas the cost of housing support decreased with AD severity.</p><p><strong>Conclusions: </strong>This is the first study estimating annual costs in people with AD from MCI to severe AD, including those for the amyloid-positive population. The study provides cost estimates by AD severity, cost components, care settings, sex, and age groups, allowing health economic modelers to apply the costs based on different model structures and populations.</p>\",\"PeriodicalId\":19807,\"journal\":{\"name\":\"PharmacoEconomics\",\"volume\":\" \",\"pages\":\"153-169\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11782292/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PharmacoEconomics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40273-024-01443-2\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40273-024-01443-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
摘要
背景:早期阿尔茨海默病(AD)诊断和治疗干预措施的发展要求对这些干预措施进行经济评估。目前仍缺乏对早期阿尔茨海默病,尤其是淀粉样蛋白阳性人群的资源利用率和成本估算。我们旨在提供与疾病严重程度相关的 AD 成本估算,并将其与对照人群进行比较。我们还旨在为临床诊断和淀粉样蛋白阳性确诊的 AD 患者提供成本估算:这是一项利用国家登记数据对资源利用情况进行的回顾性纵向分析。来自瑞典国家认知/痴呆症登记处(SveDem)的队列包括2013年至2020年间所有临床诊断为AD的患者。研究人群包括31951名AD患者和63902名年龄和性别匹配的对照者(1:2)。研究人员对这些人群进行了随访,直至其死亡、2020 年 12 月底或最后一次就诊后 2 年。直接医疗成本和社会成本是根据其他国家的登记资料估算得出的。直接医疗成本包括药物、住院和门诊费用。直接社会成本包括住院、家庭护理、短期护理、日间活动支持和住房支持的成本。年平均成本和95%置信区间通过引导法得出,以2021年瑞典克朗(SEK)为单位(2021年1瑞典克朗=0.117美元,1瑞典克朗=0.0985欧元),并按AD严重程度、成本构成、性别、年龄组和护理环境进行分类:临床确诊的注意力缺失症患者的平均年费用分别为 99,906 瑞典克朗、290,972 瑞典克朗、479,524 瑞典克朗,轻度认知障碍 (MCI)、轻度、中度和重度注意力缺失症患者的平均年费用分别为 795,617 瑞典克朗。同时获得临床诊断和淀粉样蛋白阳性 AD 确诊的人群(N = 5610)中,MCI、轻度、中度和重度 AD 的年平均费用分别为 57,625 瑞典克朗、179,153 瑞典克朗、333,095 瑞典克朗和 668,073 瑞典克朗。住院患者的年平均费用高于非住院患者,女性高于男性,年龄组高于年轻组。在所有注意力缺失症严重程度阶段,住院和药物费用相似,但门诊费用随着注意力缺失症严重程度的增加而降低。住院、家庭护理、日间活动支持和短期护理的费用随着注意力缺失症的严重程度而增加,而住房支持的费用则随着注意力缺失症的严重程度而减少:这是第一项估算从 MCI 到重度 AD 患者年度成本的研究,其中包括淀粉样蛋白阳性人群的年度成本。该研究按注意力缺失症的严重程度、成本构成、护理环境、性别和年龄组提供了成本估算,使健康经济建模人员能够根据不同的模型结构和人群应用成本。
Costs of Care in Relation to Alzheimer's Disease Severity in Sweden: A National Registry-Based Cohort Study.
Background: The advancement of diagnostic and therapeutic interventions in early Alzheimer's disease (AD) has demanded the economic evaluation of such interventions. Resource utilization and cost estimates in early AD and, more specifically, the amyloid-positive population are still lacking. We aimed to provide cost estimates in AD in relation to disease severity and compare these with the control population. We also aimed to provide cost estimates for a subset of the AD population with both clinical diagnosis and amyloid-positive confirmation.
Materials and methods: This was a retrospective longitudinal analysis of resource utilization using data from national registries. A cohort from the national Swedish registry for cognitive/dementia disorders (SveDem) includes all clinically diagnosed AD between 2013 and 2020. The study population included 31,951 people with AD and 63,902 age- and sex-matched controls (1:2). The population was followed until death, the end of December 2020, or 2 years from the last clinic visit. Direct medical and social costs were estimated from other national registries. Direct medical costs include costs for medications and inpatient and outpatient clinical visits. Direct social costs include costs for institutionalization, home care, short-term care, support for daytime activities, and housing support. Mean annual costs and 95% confidence intervals were obtained by bootstrapping, presented in 2021 Swedish Krona (SEK) (1 SEK = 0.117 USD, 1 SEK = 0.0985 EUR in 2021), and disaggregated by AD severity, cost component, sex, age group, and care setting.
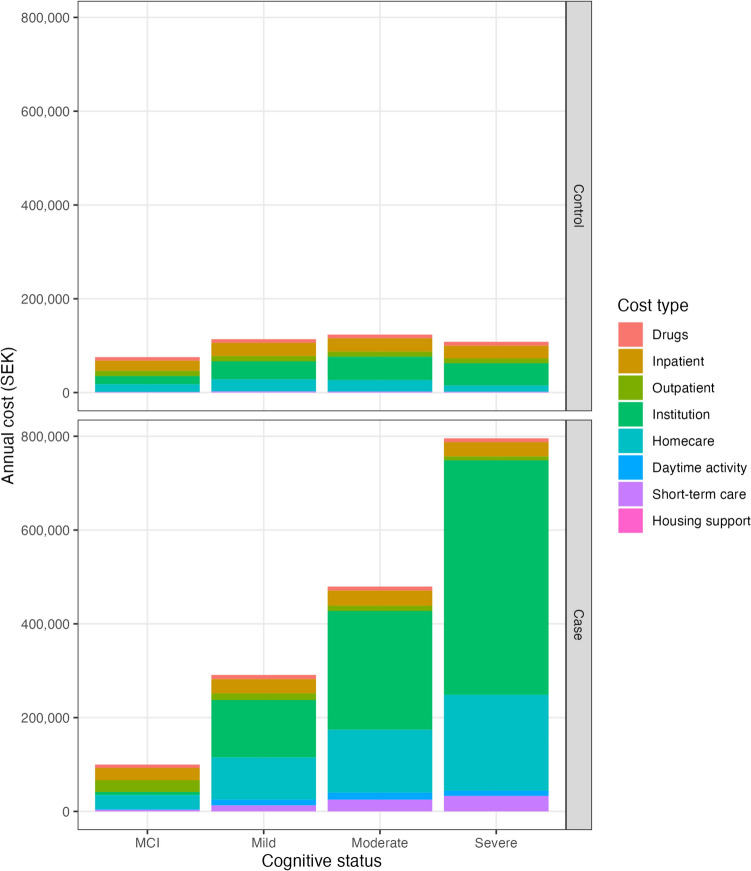
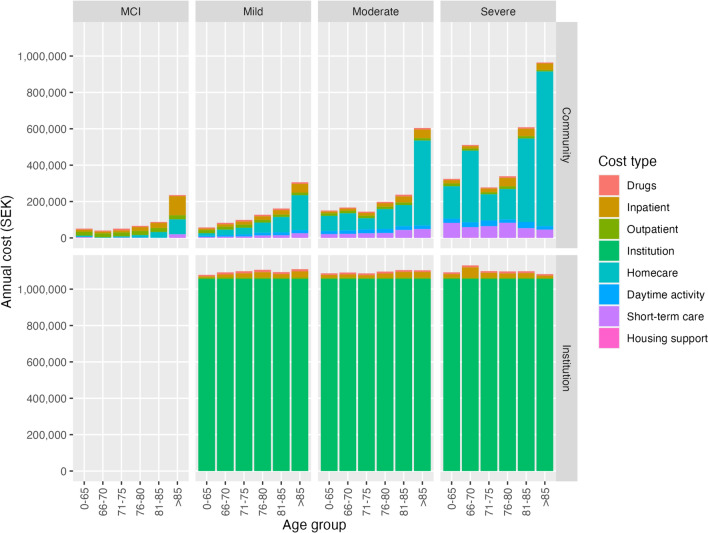
Results: Mean annual costs for individuals with clinically diagnosed AD were SEK 99,906, SEK 290,972, SEK 479,524, and SEK 795,617 in mild cognitive impairment (MCI), mild, moderate, and severe AD. The mean annual costs for the population with both clinical diagnosis and amyloid-positive AD confirmation (N = 5610) were SEK 57,625, SEK 179,153, SEK 333,095, and SEK 668,073 in MCI, mild, moderate, and severe AD, respectively. The mean annual costs were higher in institutionalized than non-institutionalized patients, females than males, and older than younger age groups. Inpatient and drug costs were similar in all AD severity stages, but outpatient costs decreased with AD severity. Costs for institutionalization, home care, support for daytime activities, and short-term care increased with AD severity, whereas the cost of housing support decreased with AD severity.
Conclusions: This is the first study estimating annual costs in people with AD from MCI to severe AD, including those for the amyloid-positive population. The study provides cost estimates by AD severity, cost components, care settings, sex, and age groups, allowing health economic modelers to apply the costs based on different model structures and populations.
期刊介绍:
PharmacoEconomics is the benchmark journal for peer-reviewed, authoritative and practical articles on the application of pharmacoeconomics and quality-of-life assessment to optimum drug therapy and health outcomes. An invaluable source of applied pharmacoeconomic original research and educational material for the healthcare decision maker.
PharmacoEconomics is dedicated to the clear communication of complex pharmacoeconomic issues related to patient care and drug utilization.
PharmacoEconomics offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
