Takeshi Onoue, Andrew H Matthews, Azin Vakilpour, Yu Kang, Bénédicte Lefebvre, Amanda M Smith, Shannon R McCurdy, Michael G Fradley, Joseph Carver, Jesse Chittams, Marielle Scherrer-Crosbie
{"title":"venetoclax对急性髓性白血病患者的心脏毒性:与蒽环类药物的比较。","authors":"Takeshi Onoue, Andrew H Matthews, Azin Vakilpour, Yu Kang, Bénédicte Lefebvre, Amanda M Smith, Shannon R McCurdy, Michael G Fradley, Joseph Carver, Jesse Chittams, Marielle Scherrer-Crosbie","doi":"10.1186/s40959-024-00275-5","DOIUrl":null,"url":null,"abstract":"<p><p>Venetoclax is a promising drug for patients with acute myeloid leukemia (AML) ineligible for anthracycline-based treatments. In rats, venetoclax is reported to cause myocardial injury. Our objectives were to report the frequency of cardiovascular (CV) events in patients treated with venetoclax, and, subsequently, to compare CV outcomes in matched patients treated with venetoclax or anthracyclines. Patients diagnosed with AML and treated with venetoclax or anthracyclines from January 2017 to July 2021 were identified. Major adverse cardiac events (MACE, including new-onset heart failure (HF), acute myocardial infarction, new onset atrial fibrillation (AF)) were recorded. Propensity-score method was then used to compare patients treated with venetoclax or anthracyclines. Patients treated with venetoclax (n=103) were older, with more hyperlipidemia than patients treated with anthracyclines (n=217). However, only 63% of patients treated with venetoclax underwent echocardiographic screening (vs. 93% of patients treated with anthracyclines, P< 0.001). Eighteen patients with venetoclax (17%) and 27 patients with anthracyclines (12%) developed MACE, including 10 % of new HF in each group. The median time to MACE was 8 days (interquartile range 5-98 days). In the matched cohort (n=132 patients), the cumulative incidence of MACE at one year was not different (17.5 % venetoclax, 9.2% anthracyclines, p =0.27). Thus, MACE incidence is similar in matched patients receiving venetoclax or anthracyclines. Close CV monitoring during the early phase of treatment may be helpful in patients treated with venetoclax.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"75"},"PeriodicalIF":3.2000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11529003/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cardiotoxicity of venetoclax in patients with acute myeloid leukemia: comparison with anthracyclines.\",\"authors\":\"Takeshi Onoue, Andrew H Matthews, Azin Vakilpour, Yu Kang, Bénédicte Lefebvre, Amanda M Smith, Shannon R McCurdy, Michael G Fradley, Joseph Carver, Jesse Chittams, Marielle Scherrer-Crosbie\",\"doi\":\"10.1186/s40959-024-00275-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Venetoclax is a promising drug for patients with acute myeloid leukemia (AML) ineligible for anthracycline-based treatments. In rats, venetoclax is reported to cause myocardial injury. Our objectives were to report the frequency of cardiovascular (CV) events in patients treated with venetoclax, and, subsequently, to compare CV outcomes in matched patients treated with venetoclax or anthracyclines. Patients diagnosed with AML and treated with venetoclax or anthracyclines from January 2017 to July 2021 were identified. Major adverse cardiac events (MACE, including new-onset heart failure (HF), acute myocardial infarction, new onset atrial fibrillation (AF)) were recorded. Propensity-score method was then used to compare patients treated with venetoclax or anthracyclines. Patients treated with venetoclax (n=103) were older, with more hyperlipidemia than patients treated with anthracyclines (n=217). However, only 63% of patients treated with venetoclax underwent echocardiographic screening (vs. 93% of patients treated with anthracyclines, P< 0.001). Eighteen patients with venetoclax (17%) and 27 patients with anthracyclines (12%) developed MACE, including 10 % of new HF in each group. The median time to MACE was 8 days (interquartile range 5-98 days). In the matched cohort (n=132 patients), the cumulative incidence of MACE at one year was not different (17.5 % venetoclax, 9.2% anthracyclines, p =0.27). Thus, MACE incidence is similar in matched patients receiving venetoclax or anthracyclines. Close CV monitoring during the early phase of treatment may be helpful in patients treated with venetoclax.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"10 1\",\"pages\":\"75\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11529003/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-024-00275-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00275-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cardiotoxicity of venetoclax in patients with acute myeloid leukemia: comparison with anthracyclines.
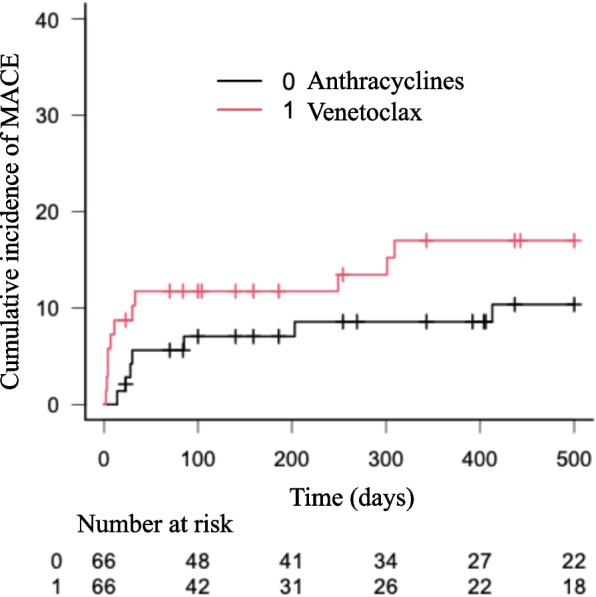
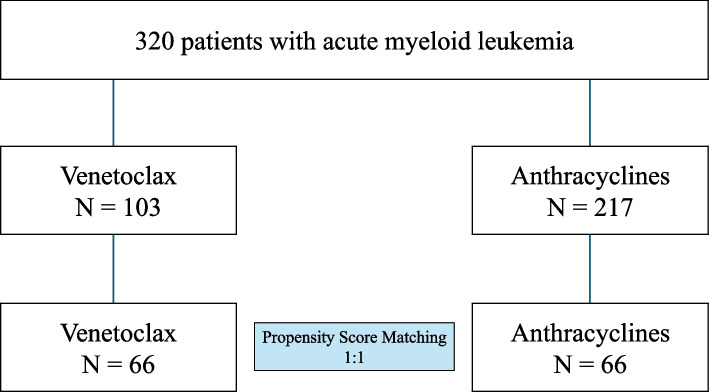
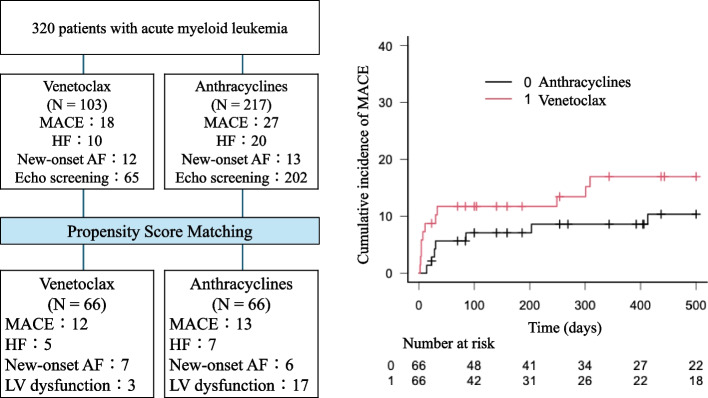
Venetoclax is a promising drug for patients with acute myeloid leukemia (AML) ineligible for anthracycline-based treatments. In rats, venetoclax is reported to cause myocardial injury. Our objectives were to report the frequency of cardiovascular (CV) events in patients treated with venetoclax, and, subsequently, to compare CV outcomes in matched patients treated with venetoclax or anthracyclines. Patients diagnosed with AML and treated with venetoclax or anthracyclines from January 2017 to July 2021 were identified. Major adverse cardiac events (MACE, including new-onset heart failure (HF), acute myocardial infarction, new onset atrial fibrillation (AF)) were recorded. Propensity-score method was then used to compare patients treated with venetoclax or anthracyclines. Patients treated with venetoclax (n=103) were older, with more hyperlipidemia than patients treated with anthracyclines (n=217). However, only 63% of patients treated with venetoclax underwent echocardiographic screening (vs. 93% of patients treated with anthracyclines, P< 0.001). Eighteen patients with venetoclax (17%) and 27 patients with anthracyclines (12%) developed MACE, including 10 % of new HF in each group. The median time to MACE was 8 days (interquartile range 5-98 days). In the matched cohort (n=132 patients), the cumulative incidence of MACE at one year was not different (17.5 % venetoclax, 9.2% anthracyclines, p =0.27). Thus, MACE incidence is similar in matched patients receiving venetoclax or anthracyclines. Close CV monitoring during the early phase of treatment may be helpful in patients treated with venetoclax.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
