Syed Hasham Ali, Zoaib Habib Tharwani, Asad Ali Siddiqui, Fizza Iqbal, Mahnoor Sadiq, Ali Abdullah, Abdullah Khalid, Huzaifa Ul Haq Ansari, Muhammad Usman, Shurjeel Uddin Qazi, Uzair Munaf, Ibtehaj Ul Haque, Shayan Marsia
{"title":"减压开颅术与开颅术治疗急性硬膜下血肿:系统综述和荟萃分析及调整亚组分析。","authors":"Syed Hasham Ali, Zoaib Habib Tharwani, Asad Ali Siddiqui, Fizza Iqbal, Mahnoor Sadiq, Ali Abdullah, Abdullah Khalid, Huzaifa Ul Haq Ansari, Muhammad Usman, Shurjeel Uddin Qazi, Uzair Munaf, Ibtehaj Ul Haque, Shayan Marsia","doi":"10.1177/11795735241297250","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute subdural hematomas are major causes of morbidity which warrant immediate treatment. If surgical intervention is warranted, craniotomy (CO) and decompressive craniectomy (DC) are employed, largely based on a loosely defined criteria and the neurosurgeon's best judgment. The primacy of one approach over another is a matter of dispute.</p><p><strong>Objective: </strong>We attempt to further clarify any advantages in the two techniques, and include a propensity score matched (PSM) subgroup analysis to eliminate bias.</p><p><strong>Design: </strong>This meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.</p><p><strong>Data sources and methods: </strong>A literature review was conducted on PubMed/Medline, Cochrane Central, and Google Scholar from inception to September 2023. 15 studies were extracted, and three outcomes were meta-analyzed: Mortality, Glasgow Outcome Scale (GOS) scores and patients undergoing re-operations/revisions. Odds Ratios (OR) and Mean Difference (MD) were used in dichotomous and continuous variables respectively. PSM data was used wherever possible. A subgroup analysis was conducted with 5 PSM studies and a trial. Heterogeneity was addressed if above 40% and the <i>P</i>-value is significant (≤ .05).</p><p><strong>Results: </strong>A total of 15 studies were meta-analyzed with a total of 2327 and 2171 patients undergoing CO and DC respectively. Patients undergoing DC had a significantly worse GOS 5 outcome (OR: .63 [95% CI: .45-.87]; <i>P</i> = .005; I2 = 0%) and higher mortality (OR: 1.58 [95% CI: 1.20-2.08]; <i>P</i> = .001; I2 = 67%). In subgroup analysis of adjusted studies, DC still had significantly higher mortality. (OR: 1.50 [95% CI: 1.03-2.18]; <i>P</i> = .001; I2 = 83%).</p><p><strong>Conclusions: </strong>This meta-analysis determines that CO is more viable than DC as a surgical option due to its less invasive nature. DC can be employed, albeit under strict preprocedural patient selection and for highly specific indications.</p>","PeriodicalId":15218,"journal":{"name":"Journal of Central Nervous System Disease","volume":"16 ","pages":"11795735241297250"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533180/pdf/","citationCount":"0","resultStr":"{\"title\":\"Decompressive craniectomy versus craniotomy for acute subdural hematoma: A systematic review and meta-analysis with an adjusted subgroup analysis.\",\"authors\":\"Syed Hasham Ali, Zoaib Habib Tharwani, Asad Ali Siddiqui, Fizza Iqbal, Mahnoor Sadiq, Ali Abdullah, Abdullah Khalid, Huzaifa Ul Haq Ansari, Muhammad Usman, Shurjeel Uddin Qazi, Uzair Munaf, Ibtehaj Ul Haque, Shayan Marsia\",\"doi\":\"10.1177/11795735241297250\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Acute subdural hematomas are major causes of morbidity which warrant immediate treatment. If surgical intervention is warranted, craniotomy (CO) and decompressive craniectomy (DC) are employed, largely based on a loosely defined criteria and the neurosurgeon's best judgment. The primacy of one approach over another is a matter of dispute.</p><p><strong>Objective: </strong>We attempt to further clarify any advantages in the two techniques, and include a propensity score matched (PSM) subgroup analysis to eliminate bias.</p><p><strong>Design: </strong>This meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.</p><p><strong>Data sources and methods: </strong>A literature review was conducted on PubMed/Medline, Cochrane Central, and Google Scholar from inception to September 2023. 15 studies were extracted, and three outcomes were meta-analyzed: Mortality, Glasgow Outcome Scale (GOS) scores and patients undergoing re-operations/revisions. Odds Ratios (OR) and Mean Difference (MD) were used in dichotomous and continuous variables respectively. PSM data was used wherever possible. A subgroup analysis was conducted with 5 PSM studies and a trial. Heterogeneity was addressed if above 40% and the <i>P</i>-value is significant (≤ .05).</p><p><strong>Results: </strong>A total of 15 studies were meta-analyzed with a total of 2327 and 2171 patients undergoing CO and DC respectively. Patients undergoing DC had a significantly worse GOS 5 outcome (OR: .63 [95% CI: .45-.87]; <i>P</i> = .005; I2 = 0%) and higher mortality (OR: 1.58 [95% CI: 1.20-2.08]; <i>P</i> = .001; I2 = 67%). In subgroup analysis of adjusted studies, DC still had significantly higher mortality. (OR: 1.50 [95% CI: 1.03-2.18]; <i>P</i> = .001; I2 = 83%).</p><p><strong>Conclusions: </strong>This meta-analysis determines that CO is more viable than DC as a surgical option due to its less invasive nature. DC can be employed, albeit under strict preprocedural patient selection and for highly specific indications.</p>\",\"PeriodicalId\":15218,\"journal\":{\"name\":\"Journal of Central Nervous System Disease\",\"volume\":\"16 \",\"pages\":\"11795735241297250\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-11-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533180/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Central Nervous System Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/11795735241297250\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Central Nervous System Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795735241297250","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
导言:急性硬膜下血肿是发病的主要原因,需要立即治疗。如果有必要进行手术治疗,可采用开颅术(CO)和减压开颅术(DC),这主要是根据松散定义的标准和神经外科医生的最佳判断。关于哪种方法优于另一种方法的问题一直存在争议:我们试图进一步澄清这两种技术的优势,并进行倾向评分匹配(PSM)亚组分析以消除偏倚:这项荟萃分析是根据系统综述和荟萃分析首选报告项目(PRISMA)指南进行的:我们在 PubMed/Medline、Cochrane Central 和 Google Scholar 上进行了文献综述,时间跨度从开始到 2023 年 9 月。提取了 15 项研究,并对三项结果进行了荟萃分析:死亡率、格拉斯哥结果量表(GOS)评分和再次手术/翻修患者。在二分变量和连续变量中分别使用了比值比(OR)和平均差(MD)。尽可能使用 PSM 数据。对 5 项 PSM 研究和一项试验进行了分组分析。如果异质性超过 40%,且 P 值显著(≤ .05),则对异质性进行处理:共对 15 项研究进行了荟萃分析,接受 CO 和 DC 治疗的患者人数分别为 2327 人和 2171 人。接受 DC 治疗的患者的 GOS 5 结果明显更差(OR:.63 [95% CI:.45-.87];P = .005;I2 = 0%),死亡率更高(OR:1.58 [95% CI:1.20-2.08];P = .001;I2 = 67%)。在对调整后的研究进行的亚组分析中,直流电的死亡率仍然显著较高。(OR:1.50 [95% CI:1.03-2.18];P = .001;I2 = 83%):这项荟萃分析表明,CO 作为一种手术选择比 DC 更为可行,因为其创伤更小。尽管需要对患者进行严格的术前选择,并针对高度特定的适应症,但直流电手术还是可以采用的。
Decompressive craniectomy versus craniotomy for acute subdural hematoma: A systematic review and meta-analysis with an adjusted subgroup analysis.
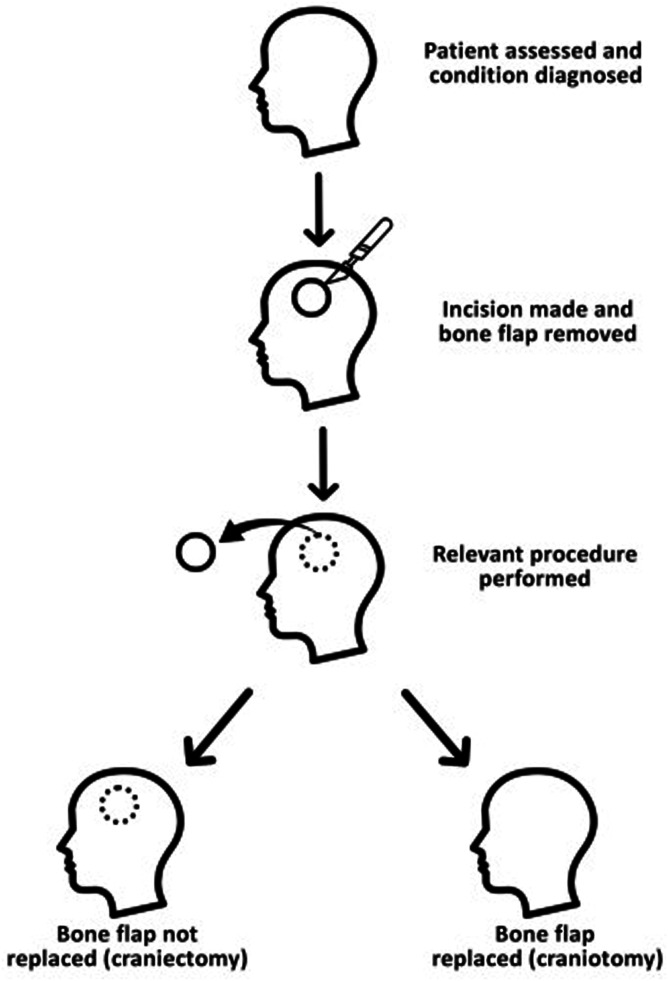
Introduction: Acute subdural hematomas are major causes of morbidity which warrant immediate treatment. If surgical intervention is warranted, craniotomy (CO) and decompressive craniectomy (DC) are employed, largely based on a loosely defined criteria and the neurosurgeon's best judgment. The primacy of one approach over another is a matter of dispute.
Objective: We attempt to further clarify any advantages in the two techniques, and include a propensity score matched (PSM) subgroup analysis to eliminate bias.
Design: This meta-analysis was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.
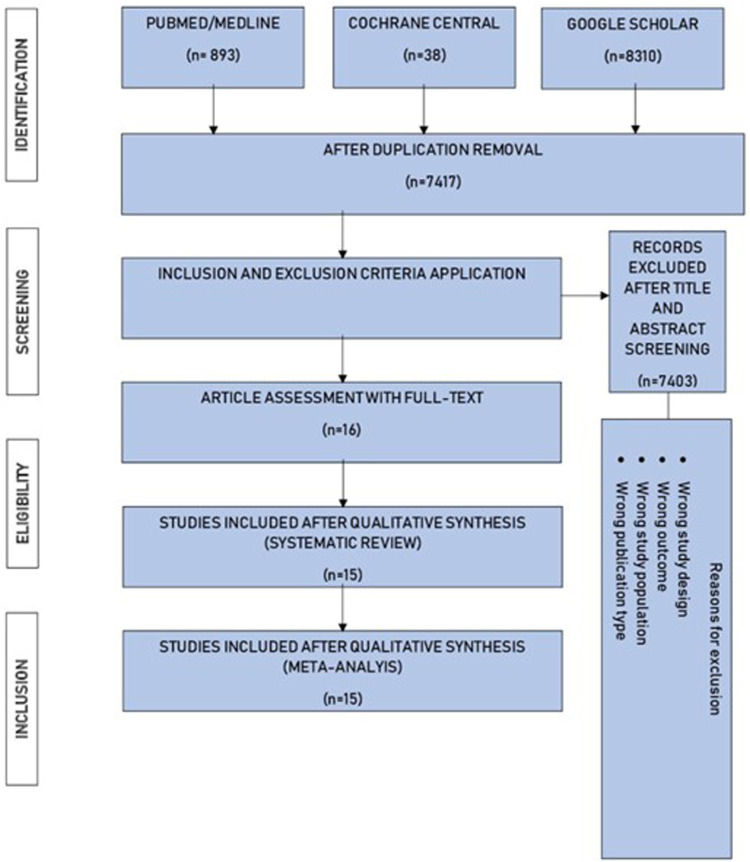
Data sources and methods: A literature review was conducted on PubMed/Medline, Cochrane Central, and Google Scholar from inception to September 2023. 15 studies were extracted, and three outcomes were meta-analyzed: Mortality, Glasgow Outcome Scale (GOS) scores and patients undergoing re-operations/revisions. Odds Ratios (OR) and Mean Difference (MD) were used in dichotomous and continuous variables respectively. PSM data was used wherever possible. A subgroup analysis was conducted with 5 PSM studies and a trial. Heterogeneity was addressed if above 40% and the P-value is significant (≤ .05).
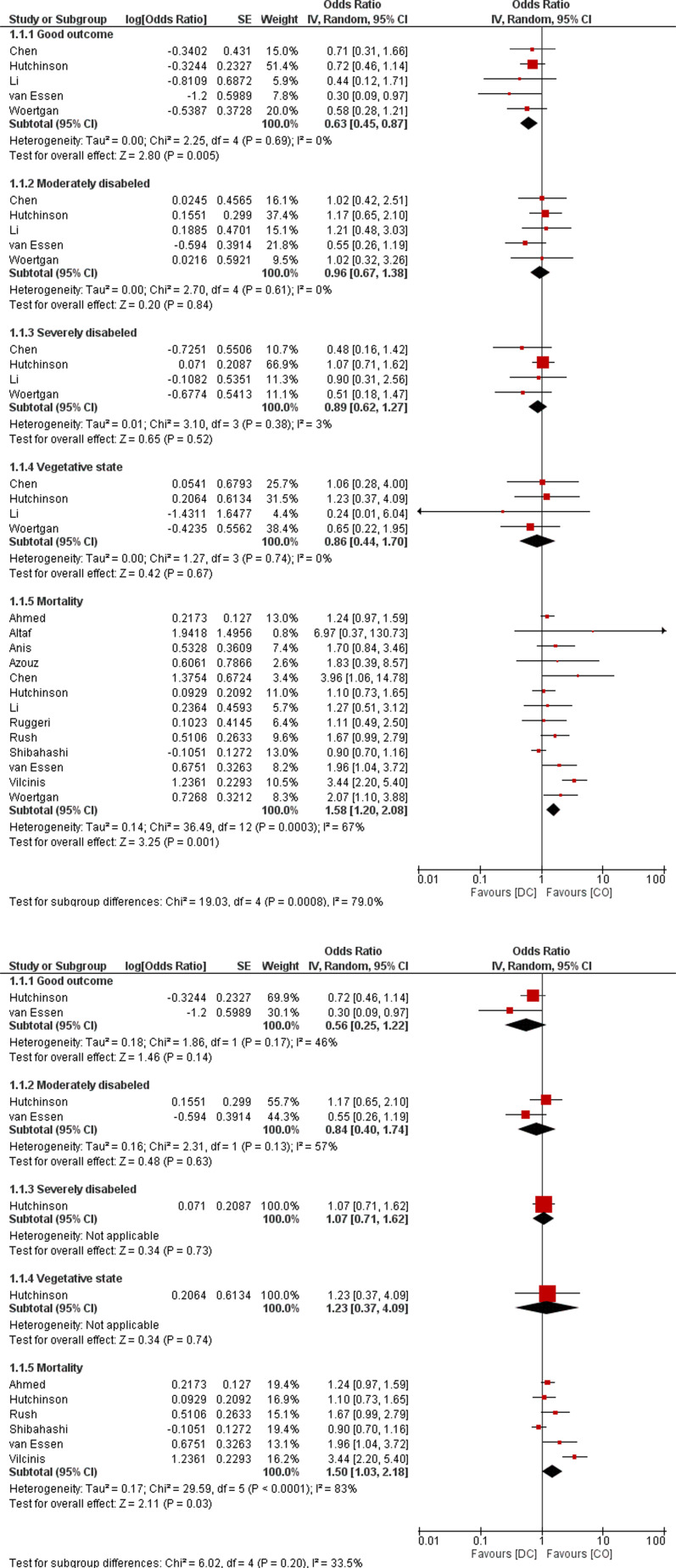
Results: A total of 15 studies were meta-analyzed with a total of 2327 and 2171 patients undergoing CO and DC respectively. Patients undergoing DC had a significantly worse GOS 5 outcome (OR: .63 [95% CI: .45-.87]; P = .005; I2 = 0%) and higher mortality (OR: 1.58 [95% CI: 1.20-2.08]; P = .001; I2 = 67%). In subgroup analysis of adjusted studies, DC still had significantly higher mortality. (OR: 1.50 [95% CI: 1.03-2.18]; P = .001; I2 = 83%).
Conclusions: This meta-analysis determines that CO is more viable than DC as a surgical option due to its less invasive nature. DC can be employed, albeit under strict preprocedural patient selection and for highly specific indications.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
