{"title":"在重症监护病房中,与格拉斯哥昏迷量表相比,无反应全纲评分的预测效力:系统综述。","authors":"Jaime E Schey, Monica Schoch, Debra Kerr","doi":"10.1007/s12028-024-02150-8","DOIUrl":null,"url":null,"abstract":"<p><p>The Full Outline of UnResponsiveness (FOUR) score was developed to overcome the limitations of the Glasgow Coma Scale (GCS) when assessing individuals with impaired consciousness. We sought to review the evidence regarding the predictive validity of the GCS and FOUR score in intensive care unit (ICU) settings. This review was prospectively registered in PROSPERO (CRD42023420528). Systematic searches of CINAHL, MEDLINE, and Embase were undertaken. Prospective observational studies were included if both GCS and FOUR score were assessed in adults during ICU admission and if mortality and/or validated functional outcome measure scores were collected. Studies were excluded if they exclusively investigated patients with traumatic brain injury. Screening, data extraction, and quality assessment using the Quality in Prognosis Studies tool were conducted by two reviewers. Twenty studies of poor to moderate quality were included. Many studies only included patients with neurological illness and excluded sedated patients, despite high proportions of intubated patients. The FOUR score achieved higher area under the receiver operating characteristic curve values for mortality prediction compared with the GCS, and the FOUR score achieved significantly higher area under the receiver operating characteristic curve values for predictions of ICU mortality. Both coma scales showed similar accuracy in predicting \"unfavorable\" functional outcome. The FOUR score appeared to be more responsive than the GCS in the ICU, as most patients with a GCS score of 3 obtained FOUR scores between 1 and 8 due to preserved brainstem function. The FOUR score may be superior to the GCS for predicting mortality in ICU settings. Further adequately powered studies with clear, reliable methods for assessment of index and outcome scores are required to clarify the predictive performance of both coma scales in ICUs. Inclusion of sedated patients may improve generalizability of findings in general ICU populations.</p>","PeriodicalId":19118,"journal":{"name":"Neurocritical Care","volume":" ","pages":"645-658"},"PeriodicalIF":3.6000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436514/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Predictive Validity of the Full Outline of UnResponsiveness Score Compared to the Glasgow Coma Scale in the Intensive Care Unit: A Systematic Review.\",\"authors\":\"Jaime E Schey, Monica Schoch, Debra Kerr\",\"doi\":\"10.1007/s12028-024-02150-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The Full Outline of UnResponsiveness (FOUR) score was developed to overcome the limitations of the Glasgow Coma Scale (GCS) when assessing individuals with impaired consciousness. We sought to review the evidence regarding the predictive validity of the GCS and FOUR score in intensive care unit (ICU) settings. This review was prospectively registered in PROSPERO (CRD42023420528). Systematic searches of CINAHL, MEDLINE, and Embase were undertaken. Prospective observational studies were included if both GCS and FOUR score were assessed in adults during ICU admission and if mortality and/or validated functional outcome measure scores were collected. Studies were excluded if they exclusively investigated patients with traumatic brain injury. Screening, data extraction, and quality assessment using the Quality in Prognosis Studies tool were conducted by two reviewers. Twenty studies of poor to moderate quality were included. Many studies only included patients with neurological illness and excluded sedated patients, despite high proportions of intubated patients. The FOUR score achieved higher area under the receiver operating characteristic curve values for mortality prediction compared with the GCS, and the FOUR score achieved significantly higher area under the receiver operating characteristic curve values for predictions of ICU mortality. Both coma scales showed similar accuracy in predicting \\\"unfavorable\\\" functional outcome. The FOUR score appeared to be more responsive than the GCS in the ICU, as most patients with a GCS score of 3 obtained FOUR scores between 1 and 8 due to preserved brainstem function. The FOUR score may be superior to the GCS for predicting mortality in ICU settings. Further adequately powered studies with clear, reliable methods for assessment of index and outcome scores are required to clarify the predictive performance of both coma scales in ICUs. Inclusion of sedated patients may improve generalizability of findings in general ICU populations.</p>\",\"PeriodicalId\":19118,\"journal\":{\"name\":\"Neurocritical Care\",\"volume\":\" \",\"pages\":\"645-658\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12436514/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurocritical Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12028-024-02150-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurocritical Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12028-024-02150-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/5 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
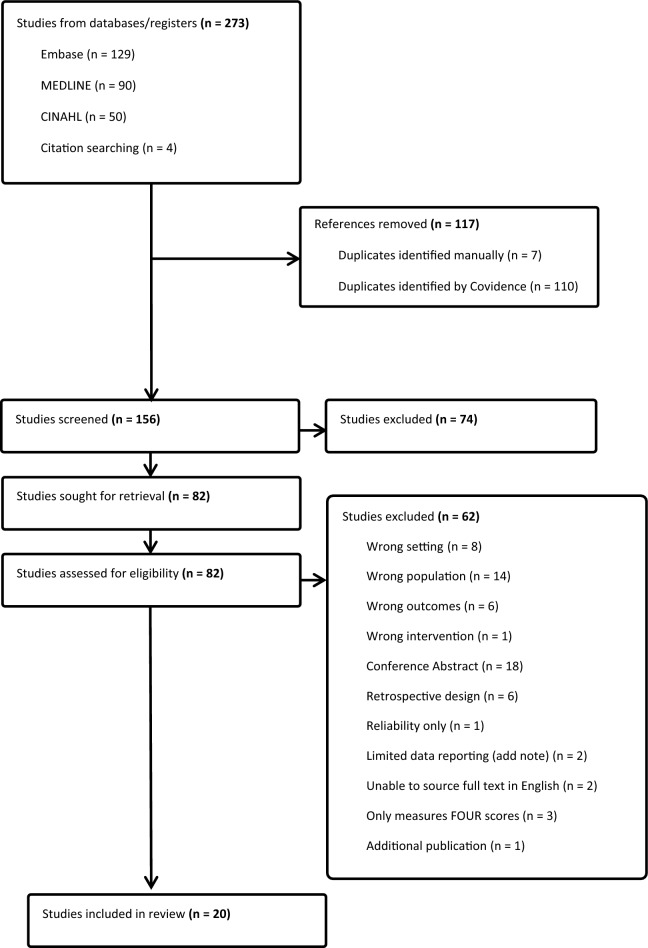
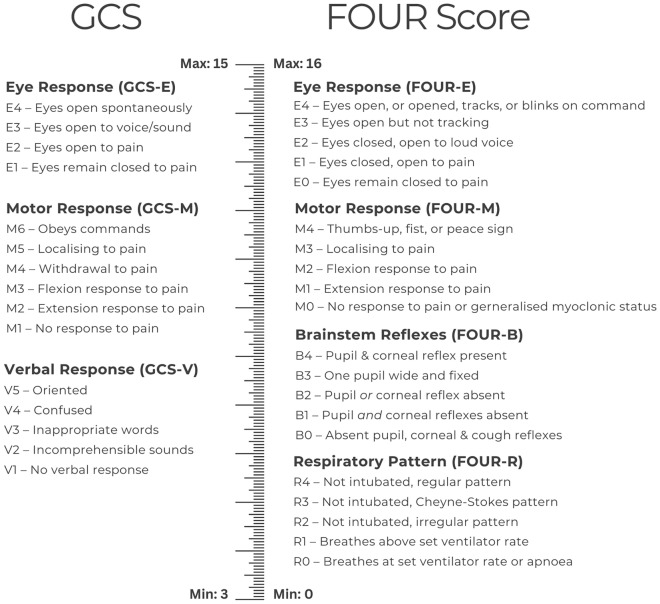
在评估意识障碍患者时,为了克服格拉斯哥昏迷量表(GCS)的局限性,我们开发了 "无反应全纲"(FOUR)评分。我们试图回顾 GCS 和 FOUR 评分在重症监护病房(ICU)环境中的预测有效性方面的证据。本综述在 PROSPERO(CRD42023420528)上进行了前瞻性注册。对 CINAHL、MEDLINE 和 Embase 进行了系统检索。纳入的前瞻性观察性研究必须同时评估成人在入住重症监护室期间的 GCS 和 FOUR 评分,并且收集了死亡率和/或有效的功能结果测量评分。如果研究仅调查脑外伤患者,则排除在外。筛选、数据提取以及使用预后研究质量工具进行的质量评估由两名审稿人完成。共纳入了 20 项质量较差至中等的研究。尽管插管患者比例较高,但许多研究仅纳入了神经系统疾病患者,并排除了镇静患者。与 GCS 相比,FOUR 评分预测死亡率的接收者操作特征曲线下面积值更高,而 FOUR 评分预测 ICU 死亡率的接收者操作特征曲线下面积值明显更高。两种昏迷量表在预测 "不利 "功能预后方面的准确性相似。在重症监护室中,FOUR评分似乎比GCS更灵敏,因为大多数GCS评分为3分的患者由于脑干功能保留,FOUR评分在1到8分之间。在 ICU 环境中,FOUR 评分在预测死亡率方面可能优于 GCS。要明确两种昏迷量表在重症监护室中的预测性能,还需要进一步开展具有明确、可靠的指数和结果评分评估方法的充分研究。纳入镇静患者可提高研究结果在普通重症监护病房人群中的通用性。
The Predictive Validity of the Full Outline of UnResponsiveness Score Compared to the Glasgow Coma Scale in the Intensive Care Unit: A Systematic Review.
The Full Outline of UnResponsiveness (FOUR) score was developed to overcome the limitations of the Glasgow Coma Scale (GCS) when assessing individuals with impaired consciousness. We sought to review the evidence regarding the predictive validity of the GCS and FOUR score in intensive care unit (ICU) settings. This review was prospectively registered in PROSPERO (CRD42023420528). Systematic searches of CINAHL, MEDLINE, and Embase were undertaken. Prospective observational studies were included if both GCS and FOUR score were assessed in adults during ICU admission and if mortality and/or validated functional outcome measure scores were collected. Studies were excluded if they exclusively investigated patients with traumatic brain injury. Screening, data extraction, and quality assessment using the Quality in Prognosis Studies tool were conducted by two reviewers. Twenty studies of poor to moderate quality were included. Many studies only included patients with neurological illness and excluded sedated patients, despite high proportions of intubated patients. The FOUR score achieved higher area under the receiver operating characteristic curve values for mortality prediction compared with the GCS, and the FOUR score achieved significantly higher area under the receiver operating characteristic curve values for predictions of ICU mortality. Both coma scales showed similar accuracy in predicting "unfavorable" functional outcome. The FOUR score appeared to be more responsive than the GCS in the ICU, as most patients with a GCS score of 3 obtained FOUR scores between 1 and 8 due to preserved brainstem function. The FOUR score may be superior to the GCS for predicting mortality in ICU settings. Further adequately powered studies with clear, reliable methods for assessment of index and outcome scores are required to clarify the predictive performance of both coma scales in ICUs. Inclusion of sedated patients may improve generalizability of findings in general ICU populations.
期刊介绍:
Neurocritical Care is a peer reviewed scientific publication whose major goal is to disseminate new knowledge on all aspects of acute neurological care. It is directed towards neurosurgeons, neuro-intensivists, neurologists, anesthesiologists, emergency physicians, and critical care nurses treating patients with urgent neurologic disorders. These are conditions that may potentially evolve rapidly and could need immediate medical or surgical intervention. Neurocritical Care provides a comprehensive overview of current developments in intensive care neurology, neurosurgery and neuroanesthesia and includes information about new therapeutic avenues and technological innovations. Neurocritical Care is the official journal of the Neurocritical Care Society.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
