Albi Angjeli, Tess Montada-Atin, Rosane Nisenbaum, Niki Dacouris, Michelle Nash, G V Ramesh Prasad, Jeffrey Zaltzman
{"title":"糖尿病肾移植受者使用钠-葡萄糖协同转运体-2 抑制剂 (SGLT2i) 的单中心经验。","authors":"Albi Angjeli, Tess Montada-Atin, Rosane Nisenbaum, Niki Dacouris, Michelle Nash, G V Ramesh Prasad, Jeffrey Zaltzman","doi":"10.1177/20543581241293202","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sodium-glucose co-tranporter-2 inhibitors have been shown to be safe and effective in patients with type 2 diabetes for improving glycemia. Furthermore large, randomized control trials have shown cardiovascular and renal benefits. However, limited safety and efficacy data is available in kidney transplant patients with diabetes.</p><p><strong>Objective: </strong>To investigate the safety and efficacy of SGLT2i use on stability of renal function in adult kidney transplant recipients (KTR) with type 2 diabetes mellitus (DM2) or New Onset Diabetes After Transplantation (NODAT).</p><p><strong>Design: </strong>We performed a single center, retrospective cohort study pre- and post-SGLT2i exposure.</p><p><strong>Patients: </strong>Adults with DM2 or NODAT who received a living or deceased kidney transplant (Tx) and started on an SGLT2i post-Tx were reviewed. Patients who had type 1 diabetes were excluded.</p><p><strong>Measurements and methods: </strong>The baseline was the SGLT2i start date. We reviewed available data from 24 months (M) before and after SGLT2i initiation. The primary endpoints were the effects of SGLT2i use on stability of renal function using serum creatinine and eGFR, change in urine albumin excretion(uACR), and glycosylated hemoglobin (A1C). Secondary endpoints compared blood pressure, body mass index and adverse reactions at baseline and quarterly after SGLT2i initiation.</p><p><strong>Results: </strong>125 KTRs were included in cohort: NODAT (52, 42%), DM2 (73, 58%); female (33, 27%); mean age at Tx 55 years (25-75); LD (56, 45%), DD (69, 55%); mean duration of Tx (6.8 years, 0.1-42.5); study follow-up (1.8 years, 0.3-4.9).The mean eGFR remained stable pre-SGLT2i at 64.6 mL/min/1.73m<sup>2</sup>, vs post at 64.3 mL/min/1.73m<sup>2</sup>. There was no difference in mean A1C after SGLT2i initiation. The slope of uACR using natural log transformation pre-SGLT2i compared with post-SGLT2i slope reduced from +0.7 (0.03, 0.11) to -0.04 (-0.01, -0.35) mg/mmol/3mths (<i>P</i> = .002). The risk of developing new genital mycotic infections among all patients was 4% (95% CI 1.3%-9.1%) While there was no significant difference in UTI before (13.6%) and after (12%) SGLT2i use (<i>P</i> = .68), there was a higher risk of UTI seen in patients with a previous history of UTI (23.5%) vs no previous history (10.2%) post initiation. There was no significant increase in AKI pre 8%, post 10.4%, <i>P</i> = .51. There was a single DKA event pre- and post-SGLT2.</p><p><strong>Limitations: </strong>The limitations of this study include its retrospective nonrandomized nature.</p><p><strong>Conclusion: </strong>In this retrospective analysis, SGLT2i use in KTR appears to be safe and efficacious with stable renal function and glycemic control, alongside improvements in uACR. There was a low risk of new genital yeast infections after SGLT2i start. UTI occurrence was higher in patients with a previous history of UTI compared with those with no previous history.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241293202"},"PeriodicalIF":1.6000,"publicationDate":"2024-11-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555736/pdf/","citationCount":"0","resultStr":"{\"title\":\"Single Center Experience With Sodium-Glucose Co-Transporter-2 Inhibitors (SGLT2i) in Kidney Transplant Recipients With Diabetes.\",\"authors\":\"Albi Angjeli, Tess Montada-Atin, Rosane Nisenbaum, Niki Dacouris, Michelle Nash, G V Ramesh Prasad, Jeffrey Zaltzman\",\"doi\":\"10.1177/20543581241293202\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sodium-glucose co-tranporter-2 inhibitors have been shown to be safe and effective in patients with type 2 diabetes for improving glycemia. Furthermore large, randomized control trials have shown cardiovascular and renal benefits. However, limited safety and efficacy data is available in kidney transplant patients with diabetes.</p><p><strong>Objective: </strong>To investigate the safety and efficacy of SGLT2i use on stability of renal function in adult kidney transplant recipients (KTR) with type 2 diabetes mellitus (DM2) or New Onset Diabetes After Transplantation (NODAT).</p><p><strong>Design: </strong>We performed a single center, retrospective cohort study pre- and post-SGLT2i exposure.</p><p><strong>Patients: </strong>Adults with DM2 or NODAT who received a living or deceased kidney transplant (Tx) and started on an SGLT2i post-Tx were reviewed. Patients who had type 1 diabetes were excluded.</p><p><strong>Measurements and methods: </strong>The baseline was the SGLT2i start date. We reviewed available data from 24 months (M) before and after SGLT2i initiation. The primary endpoints were the effects of SGLT2i use on stability of renal function using serum creatinine and eGFR, change in urine albumin excretion(uACR), and glycosylated hemoglobin (A1C). Secondary endpoints compared blood pressure, body mass index and adverse reactions at baseline and quarterly after SGLT2i initiation.</p><p><strong>Results: </strong>125 KTRs were included in cohort: NODAT (52, 42%), DM2 (73, 58%); female (33, 27%); mean age at Tx 55 years (25-75); LD (56, 45%), DD (69, 55%); mean duration of Tx (6.8 years, 0.1-42.5); study follow-up (1.8 years, 0.3-4.9).The mean eGFR remained stable pre-SGLT2i at 64.6 mL/min/1.73m<sup>2</sup>, vs post at 64.3 mL/min/1.73m<sup>2</sup>. There was no difference in mean A1C after SGLT2i initiation. The slope of uACR using natural log transformation pre-SGLT2i compared with post-SGLT2i slope reduced from +0.7 (0.03, 0.11) to -0.04 (-0.01, -0.35) mg/mmol/3mths (<i>P</i> = .002). The risk of developing new genital mycotic infections among all patients was 4% (95% CI 1.3%-9.1%) While there was no significant difference in UTI before (13.6%) and after (12%) SGLT2i use (<i>P</i> = .68), there was a higher risk of UTI seen in patients with a previous history of UTI (23.5%) vs no previous history (10.2%) post initiation. There was no significant increase in AKI pre 8%, post 10.4%, <i>P</i> = .51. There was a single DKA event pre- and post-SGLT2.</p><p><strong>Limitations: </strong>The limitations of this study include its retrospective nonrandomized nature.</p><p><strong>Conclusion: </strong>In this retrospective analysis, SGLT2i use in KTR appears to be safe and efficacious with stable renal function and glycemic control, alongside improvements in uACR. There was a low risk of new genital yeast infections after SGLT2i start. UTI occurrence was higher in patients with a previous history of UTI compared with those with no previous history.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"11 \",\"pages\":\"20543581241293202\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-11-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555736/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581241293202\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241293202","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Single Center Experience With Sodium-Glucose Co-Transporter-2 Inhibitors (SGLT2i) in Kidney Transplant Recipients With Diabetes.
Background: Sodium-glucose co-tranporter-2 inhibitors have been shown to be safe and effective in patients with type 2 diabetes for improving glycemia. Furthermore large, randomized control trials have shown cardiovascular and renal benefits. However, limited safety and efficacy data is available in kidney transplant patients with diabetes.
Objective: To investigate the safety and efficacy of SGLT2i use on stability of renal function in adult kidney transplant recipients (KTR) with type 2 diabetes mellitus (DM2) or New Onset Diabetes After Transplantation (NODAT).
Design: We performed a single center, retrospective cohort study pre- and post-SGLT2i exposure.
Patients: Adults with DM2 or NODAT who received a living or deceased kidney transplant (Tx) and started on an SGLT2i post-Tx were reviewed. Patients who had type 1 diabetes were excluded.
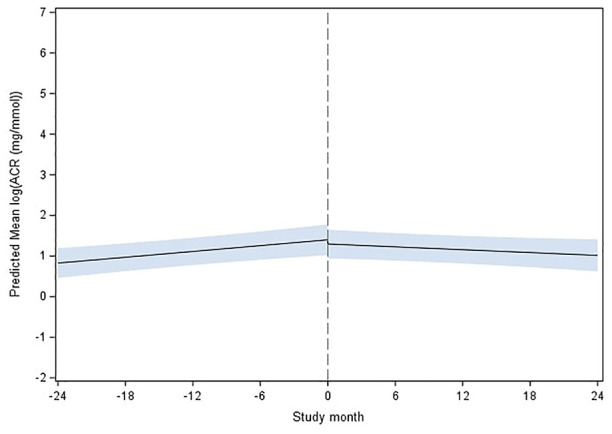
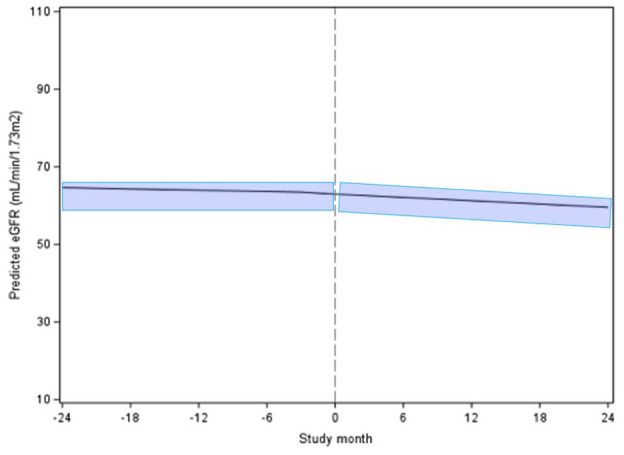
Measurements and methods: The baseline was the SGLT2i start date. We reviewed available data from 24 months (M) before and after SGLT2i initiation. The primary endpoints were the effects of SGLT2i use on stability of renal function using serum creatinine and eGFR, change in urine albumin excretion(uACR), and glycosylated hemoglobin (A1C). Secondary endpoints compared blood pressure, body mass index and adverse reactions at baseline and quarterly after SGLT2i initiation.
Results: 125 KTRs were included in cohort: NODAT (52, 42%), DM2 (73, 58%); female (33, 27%); mean age at Tx 55 years (25-75); LD (56, 45%), DD (69, 55%); mean duration of Tx (6.8 years, 0.1-42.5); study follow-up (1.8 years, 0.3-4.9).The mean eGFR remained stable pre-SGLT2i at 64.6 mL/min/1.73m2, vs post at 64.3 mL/min/1.73m2. There was no difference in mean A1C after SGLT2i initiation. The slope of uACR using natural log transformation pre-SGLT2i compared with post-SGLT2i slope reduced from +0.7 (0.03, 0.11) to -0.04 (-0.01, -0.35) mg/mmol/3mths (P = .002). The risk of developing new genital mycotic infections among all patients was 4% (95% CI 1.3%-9.1%) While there was no significant difference in UTI before (13.6%) and after (12%) SGLT2i use (P = .68), there was a higher risk of UTI seen in patients with a previous history of UTI (23.5%) vs no previous history (10.2%) post initiation. There was no significant increase in AKI pre 8%, post 10.4%, P = .51. There was a single DKA event pre- and post-SGLT2.
Limitations: The limitations of this study include its retrospective nonrandomized nature.
Conclusion: In this retrospective analysis, SGLT2i use in KTR appears to be safe and efficacious with stable renal function and glycemic control, alongside improvements in uACR. There was a low risk of new genital yeast infections after SGLT2i start. UTI occurrence was higher in patients with a previous history of UTI compared with those with no previous history.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
