Sareen Singh, Syed Sibte Raza Abidi, Syed Asil Ali Naqvi, Amanda J Vinson, Thomas A A Skinner, George Worthen, Samina Abidi, Kenneth A West, Karthik K Tennankore
{"title":"Using Unsupervised Clustering to Characterize Phenotypes Among Older Kidney Transplant Recipients: A Cohort Study.","authors":"Sareen Singh, Syed Sibte Raza Abidi, Syed Asil Ali Naqvi, Amanda J Vinson, Thomas A A Skinner, George Worthen, Samina Abidi, Kenneth A West, Karthik K Tennankore","doi":"10.1177/20543581251322576","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Older kidney transplant recipients have inferior outcomes compared to younger recipients, and this risk may be compounded by donor characteristics.</p><p><strong>Objective: </strong>We applied an unsupervised machine learning clustering approach to group older recipients into similar phenotypes. We evaluated the association between each cluster and graft failure, and the impact of donor quality on outcomes.</p><p><strong>Design: </strong>This is a nationally representative retrospective cohort study.</p><p><strong>Setting and patients: </strong>Kidney transplant recipients aged ≥65 years identified from the Scientific Registry of Transplant Recipients (2000-2017).</p><p><strong>Measurements and methods: </strong>We used unsupervised clustering to generate phenotypes using 16 recipient factors. Donor quality was evaluated using 2 approaches, including the Kidney Donor Risk Index (KDRI). All-cause graft failure was analyzed using multivariable Cox regression.</p><p><strong>Results: </strong>Overall, 16 364 patients (mean age 69 years; 38% female) were separated into 3 clusters. Cluster 1 recipients were exclusively female; cluster 2 recipients were exclusively males without diabetes; and cluster 3 recipients were males with a higher burden of comorbidities. Compared to cluster 2, the risk of graft failure was higher for cluster 3 recipients (adjusted hazard ratio [aHR] = 1.25, 95% confidence interval [CI] = 1.19-1.32). Cluster 3 recipients of a lower quality (KDRI ≥1.45) kidney had the highest risk of graft failure (aHR = 1.74, 95% CI = 1.61-1.87) relative to cluster 2 recipients of a higher quality kidney.</p><p><strong>Limitations: </strong>This study did not include an external validation cohort. The findings should be interpreted as exploratory and should not be used to inform individual risk prediction nor be applied to recipients <65 years of age.</p><p><strong>Conclusions: </strong>In a national cohort of older kidney transplant recipients, unsupervised clustering generated 3 clinically distinct recipient phenotypes. These phenotypes may aid in complementing allocation decisions, providing prognostic information, and optimizing post-transplant care for older recipients.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251322576"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11909662/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251322576","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Older kidney transplant recipients have inferior outcomes compared to younger recipients, and this risk may be compounded by donor characteristics.
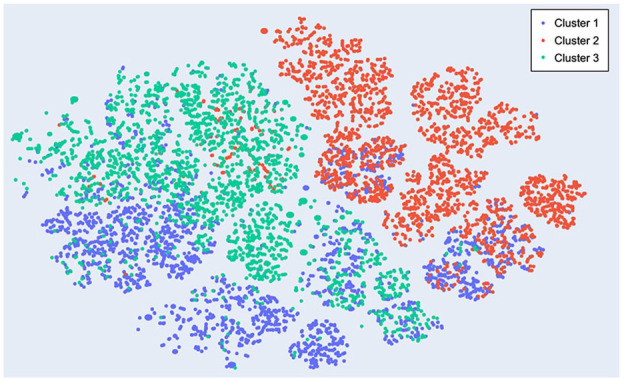
Objective: We applied an unsupervised machine learning clustering approach to group older recipients into similar phenotypes. We evaluated the association between each cluster and graft failure, and the impact of donor quality on outcomes.
Design: This is a nationally representative retrospective cohort study.
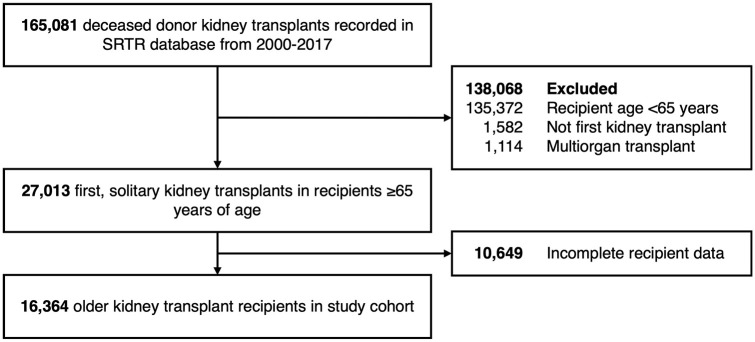
Setting and patients: Kidney transplant recipients aged ≥65 years identified from the Scientific Registry of Transplant Recipients (2000-2017).
Measurements and methods: We used unsupervised clustering to generate phenotypes using 16 recipient factors. Donor quality was evaluated using 2 approaches, including the Kidney Donor Risk Index (KDRI). All-cause graft failure was analyzed using multivariable Cox regression.
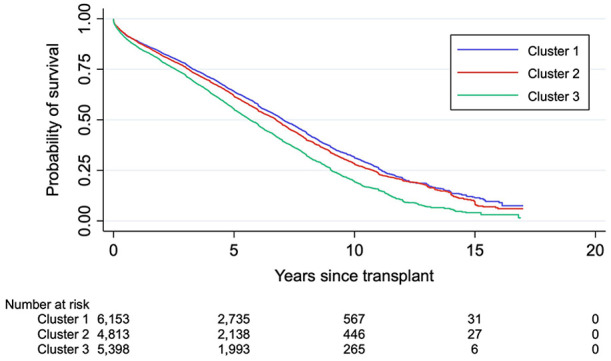
Results: Overall, 16 364 patients (mean age 69 years; 38% female) were separated into 3 clusters. Cluster 1 recipients were exclusively female; cluster 2 recipients were exclusively males without diabetes; and cluster 3 recipients were males with a higher burden of comorbidities. Compared to cluster 2, the risk of graft failure was higher for cluster 3 recipients (adjusted hazard ratio [aHR] = 1.25, 95% confidence interval [CI] = 1.19-1.32). Cluster 3 recipients of a lower quality (KDRI ≥1.45) kidney had the highest risk of graft failure (aHR = 1.74, 95% CI = 1.61-1.87) relative to cluster 2 recipients of a higher quality kidney.
Limitations: This study did not include an external validation cohort. The findings should be interpreted as exploratory and should not be used to inform individual risk prediction nor be applied to recipients <65 years of age.
Conclusions: In a national cohort of older kidney transplant recipients, unsupervised clustering generated 3 clinically distinct recipient phenotypes. These phenotypes may aid in complementing allocation decisions, providing prognostic information, and optimizing post-transplant care for older recipients.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
