Magnus S Jørgensen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Martin Graversen
{"title":"在对无法切除的腹膜转移瘤进行 PIPAC 指导治疗期间,腹腔镜超声波的影响。","authors":"Magnus S Jørgensen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Martin Graversen","doi":"10.1515/pp-2024-0007","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Laparoscopic ultrasound (LUS) combines both laparoscopy and ultrasound imaging of the peritoneum liver and retroperitoneum. LUS has not been described in treatments with pressurized intraperitoneal aerosol chemotherapy (PIPAC). We present our experience with LUS in patients undergoing PIPAC.</p><p><strong>Methods: </strong>Retrospective study of LUS findings from the prospective PIPAC-OPC2 trial. Main outcome was changes in overall treatment strategy due to LUS findings.</p><p><strong>Results: </strong>PIPAC-OPC2 included 143 patients of which 33 patients were treated with electrostatic precipitation PIPAC. Nine patients were excluded due to primary non-access. During PIPAC 1, LUS was performed in 112 of 134 (84 %) PIPAC procedures and changed overall treatment strategy in one patient due to detection of multiple liver metastases unseen by baseline CT. During PIPAC 2 and 3 LUS was performed in 59 of 104 (57 %) and 42 of 78 (54 %) PIPAC procedures, respectively. Throughout PIPAC 1-3, LUS also detected pathological lymph nodes in 16 patients, and focal liver lesions in another four patients of uncertain origin. No further examinations were performed in these patients, and the overall treatment strategy was not changed according to the PIPAC-OPC2 protocol. One patient had a splenic capsule rupture related to the LUS itself. This was managed conservatively.</p><p><strong>Conclusions: </strong>LUS may be safely performed during PIPAC. However, LUS has limited clinical impact in patients scheduled for PIPAC, and cannot be recommended as a routine procedure when performing PIPAC.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"9 3","pages":"107-112"},"PeriodicalIF":2.4000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558172/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of laparoscopic ultrasound during PIPAC directed treatment of unresectable peritoneal metastasis.\",\"authors\":\"Magnus S Jørgensen, Alan P Ainsworth, Claus W Fristrup, Michael B Mortensen, Martin Graversen\",\"doi\":\"10.1515/pp-2024-0007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Laparoscopic ultrasound (LUS) combines both laparoscopy and ultrasound imaging of the peritoneum liver and retroperitoneum. LUS has not been described in treatments with pressurized intraperitoneal aerosol chemotherapy (PIPAC). We present our experience with LUS in patients undergoing PIPAC.</p><p><strong>Methods: </strong>Retrospective study of LUS findings from the prospective PIPAC-OPC2 trial. Main outcome was changes in overall treatment strategy due to LUS findings.</p><p><strong>Results: </strong>PIPAC-OPC2 included 143 patients of which 33 patients were treated with electrostatic precipitation PIPAC. Nine patients were excluded due to primary non-access. During PIPAC 1, LUS was performed in 112 of 134 (84 %) PIPAC procedures and changed overall treatment strategy in one patient due to detection of multiple liver metastases unseen by baseline CT. During PIPAC 2 and 3 LUS was performed in 59 of 104 (57 %) and 42 of 78 (54 %) PIPAC procedures, respectively. Throughout PIPAC 1-3, LUS also detected pathological lymph nodes in 16 patients, and focal liver lesions in another four patients of uncertain origin. No further examinations were performed in these patients, and the overall treatment strategy was not changed according to the PIPAC-OPC2 protocol. One patient had a splenic capsule rupture related to the LUS itself. This was managed conservatively.</p><p><strong>Conclusions: </strong>LUS may be safely performed during PIPAC. However, LUS has limited clinical impact in patients scheduled for PIPAC, and cannot be recommended as a routine procedure when performing PIPAC.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"9 3\",\"pages\":\"107-112\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558172/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2024-0007\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2024-0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Impact of laparoscopic ultrasound during PIPAC directed treatment of unresectable peritoneal metastasis.
Objectives: Laparoscopic ultrasound (LUS) combines both laparoscopy and ultrasound imaging of the peritoneum liver and retroperitoneum. LUS has not been described in treatments with pressurized intraperitoneal aerosol chemotherapy (PIPAC). We present our experience with LUS in patients undergoing PIPAC.
Methods: Retrospective study of LUS findings from the prospective PIPAC-OPC2 trial. Main outcome was changes in overall treatment strategy due to LUS findings.
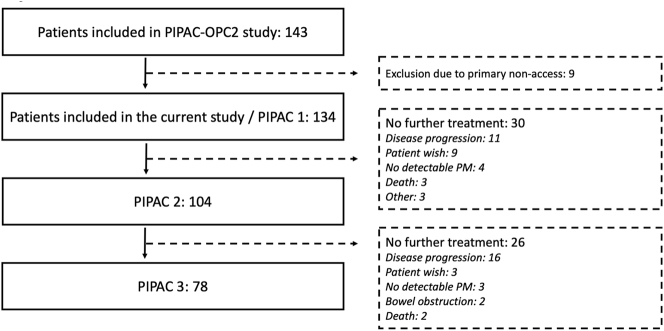
Results: PIPAC-OPC2 included 143 patients of which 33 patients were treated with electrostatic precipitation PIPAC. Nine patients were excluded due to primary non-access. During PIPAC 1, LUS was performed in 112 of 134 (84 %) PIPAC procedures and changed overall treatment strategy in one patient due to detection of multiple liver metastases unseen by baseline CT. During PIPAC 2 and 3 LUS was performed in 59 of 104 (57 %) and 42 of 78 (54 %) PIPAC procedures, respectively. Throughout PIPAC 1-3, LUS also detected pathological lymph nodes in 16 patients, and focal liver lesions in another four patients of uncertain origin. No further examinations were performed in these patients, and the overall treatment strategy was not changed according to the PIPAC-OPC2 protocol. One patient had a splenic capsule rupture related to the LUS itself. This was managed conservatively.
Conclusions: LUS may be safely performed during PIPAC. However, LUS has limited clinical impact in patients scheduled for PIPAC, and cannot be recommended as a routine procedure when performing PIPAC.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
