{"title":"哥伦比亚猕猴病诊断、预防和管理共识","authors":"Jesús Andrés Benavides-Serralde, Marcela Buitrago-Leal, Saulo Molina Giraldo, Juan Pablo Benavides Calvache, Isabella Rivera Tobar, Melva Juliana López Rodríguez, Jezid Miranda, Catalina Valencia","doi":"10.18597/rcog.4142","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To train healthcare professionals involved in the care of Rh-D negative pregnant women, with the aim of standardizing the management of Rh isoimmunization prevention, timely antenatal diagnosis of Rh disease, fetal assessment, and treatment of fetuses with Rh disease, in order to prevent adverse perinatal outcomes.</p><p><strong>Materials and methods: </strong>A group of 23 expert panelists participated in the development of the consensus through three rounds, answering a questionnaire consisting of 8 domains and 22 questions. A modified Delphi method was used until the consensus threshold among participants was reached, defined as 80% or greater agreement in responses. In the third round of the expert panel, a twenty-third question emerged, which was answered by one of the thematic leaders. The eight domains of antenatal management for Rh-D negative pregnant women were: 1) Rh-D determination, 2) initial prenatal care for Rh-D negative patients, 3) titration and periodicity of the indirect Coombs test, 4) sensitizing events, 5) administration of anti-D immunoglobulin (IgG), 6) Doppler velocimetry of the middle cerebral artery (MCA), 7) antenatal management of isoimmunized patients and anemic fetuses, and 8) timing for pregnancy termination based on different clinical scenarios. Based on these responses, and a review of international clinical practice guidelines, consensus statements were formulated, including recommendations, their justification, and adaptation to the local context.</p><p><strong>Results: </strong>The following recommendations were issued:\n\nIt is suggested that Rh-D negative women of childbearing age attend a preconception consultation.\nIt is recommended to determine maternal Rh-D status at the first contact with health services, either during the preconception consultation or at the first prenatal check-up.\nFor Rh-D negative patients, it is recommended to determine the Rh-D status of the child's father during prenatal care as early as possible, preferably before the 28th week of gestation.\nFor Rh-D negative primigravidas, where the father is Rh-D positive, it is suggested to: a) determine and quantify Rh-D antibodies (indirect Coombs test) during the first consultation and then quarterly, b) expand the obstetric history, with an emphasis on identifying sensitizing events, and c) provide parental counseling regarding potential risks, the need for additional tests, and the possibility of immunization during pregnancy.\nDuring prenatal care for Rh-D negative multiparous patients with previous Rh-D positive offspring, the initial approach should include: a) determining and titrating Rh-D antibodies (indirect Coombs test); b) expanding the obstetric history, focusing on sensitizing events; and c) providing parental counseling about potential risks and additional tests.\nAfter a sensitizing event, it is recommended to administer anti-D IgG within the first 72 hours at a dose of 1500 IU (300 μg). If not feasible, it can be administered up to 4 weeks after the event if it was not given initially.\n\n7.1. For non-isoimmunized pregnant women (with a negative Coombs test and Rh-positive newborn), it is recommended to administer anti-D IgG between weeks 28 and 32, and within the first 72 hours postpartum if the newborn is Rh-positive. The dose is 300 μg IM or IV.\n\n7.2. In the case of a cesarean section in an Rh-D negative patient with a Rh-D positive child, the consensus does not recommend doubling the dose of anti-D IgG. The dose remains the same as after a vaginal delivery: 300 μg IM or IV.\n\n7.3. In a twin delivery involving an Rh-D negative patient with two or more Rh-D positive live-born infants, the consensus recommends not doubling the dose of anti-D IgG. The dose remains 300 μg IM or IV, the same as after a vaginal delivery.\n\n7.4. For a non-isoimmunized Rh-D negative patient in the puerperium with immediate postpartum surgical tubal sterilization and an Rh-D positive neonate, anti-D IgG is recommended, assuming no prior sensitization, given the potential for reproductive decision changes or failure of the procedure.\n\nAn Rh-D negative patient is considered isoimmunized if: a) the indirect Coombs test is positive at any titer, provided anti-D IgG was not received in the previous month, or b) there is a history of adverse perinatal outcomes associated with Rh disease in prior pregnancies, such as hydrops.\n9.1. If Rh-D negative women are isoimmunized, it is necessary to determine the anti-D antibody titer, as this titer correlates with the severity of the disease and determines the need for fetal anemia studies with Doppler velocimetry of the MCA.\n\n9.2. For isoimmunized Rh-D negative patients, it is recommended to follow up with monthly quantitative indirect Coombs tests until week 24, then bi-weekly, or until reaching a critical titer (≥ 1:16).\n\n10.1. Doppler ultrasound of the MCA is suggested for Rh-D negative patients with a positive indirect Coombs test and titers ≥ 1:16.\n\n10.2. In non-isoimmunized Rh-D negative patients, the consensus does not recommend MCA Doppler velocimetry.\n\n10.3. Weekly MCA Doppler ultrasounds are recommended for isoimmunized patients with indirect Coombs titers ≥ 1:16.\n\n10.4. The consensus suggests adopting a cut-off value of ≥ 1.5 multiples of the median (MoM) of the peak systolic velocity for gestational age on MCA Doppler, as this value best correlates with fetal anemia.\n\nThe consensus suggests Cordocentesis when fetal anemia is suspected, and intrauterine fetal transfusion when cordocentesis shows severe fetal anemia. This procedure should be performed by trained personnel.\nIt is recommended to prolong pregnancy until the fetus has achieved sufficient lung and tissue maturation to improve perinatal survival, according to the indirect Coombs test titer threshold.</p><p><strong>Conclusions: </strong>It is essential to address Rh-D negative pregnant women, isoimmunized women, and fetuses with Rh disease in an appropriate and standardized manner, according to the Colombian context, across all levels of prenatal care. The recommendations issued in this consensus are expected to improve clinical care, as well as enhance perinatal health and neonatal quality of life in cases of Rh disease.</p>","PeriodicalId":101422,"journal":{"name":"Revista colombiana de obstetricia y ginecologia","volume":"75 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11457932/pdf/","citationCount":"0","resultStr":"{\"title\":\"[Colombian consensus for the diagnosis, prevention, and management of Rhesus disease].\",\"authors\":\"Jesús Andrés Benavides-Serralde, Marcela Buitrago-Leal, Saulo Molina Giraldo, Juan Pablo Benavides Calvache, Isabella Rivera Tobar, Melva Juliana López Rodríguez, Jezid Miranda, Catalina Valencia\",\"doi\":\"10.18597/rcog.4142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To train healthcare professionals involved in the care of Rh-D negative pregnant women, with the aim of standardizing the management of Rh isoimmunization prevention, timely antenatal diagnosis of Rh disease, fetal assessment, and treatment of fetuses with Rh disease, in order to prevent adverse perinatal outcomes.</p><p><strong>Materials and methods: </strong>A group of 23 expert panelists participated in the development of the consensus through three rounds, answering a questionnaire consisting of 8 domains and 22 questions. A modified Delphi method was used until the consensus threshold among participants was reached, defined as 80% or greater agreement in responses. In the third round of the expert panel, a twenty-third question emerged, which was answered by one of the thematic leaders. The eight domains of antenatal management for Rh-D negative pregnant women were: 1) Rh-D determination, 2) initial prenatal care for Rh-D negative patients, 3) titration and periodicity of the indirect Coombs test, 4) sensitizing events, 5) administration of anti-D immunoglobulin (IgG), 6) Doppler velocimetry of the middle cerebral artery (MCA), 7) antenatal management of isoimmunized patients and anemic fetuses, and 8) timing for pregnancy termination based on different clinical scenarios. Based on these responses, and a review of international clinical practice guidelines, consensus statements were formulated, including recommendations, their justification, and adaptation to the local context.</p><p><strong>Results: </strong>The following recommendations were issued:\\n\\nIt is suggested that Rh-D negative women of childbearing age attend a preconception consultation.\\nIt is recommended to determine maternal Rh-D status at the first contact with health services, either during the preconception consultation or at the first prenatal check-up.\\nFor Rh-D negative patients, it is recommended to determine the Rh-D status of the child's father during prenatal care as early as possible, preferably before the 28th week of gestation.\\nFor Rh-D negative primigravidas, where the father is Rh-D positive, it is suggested to: a) determine and quantify Rh-D antibodies (indirect Coombs test) during the first consultation and then quarterly, b) expand the obstetric history, with an emphasis on identifying sensitizing events, and c) provide parental counseling regarding potential risks, the need for additional tests, and the possibility of immunization during pregnancy.\\nDuring prenatal care for Rh-D negative multiparous patients with previous Rh-D positive offspring, the initial approach should include: a) determining and titrating Rh-D antibodies (indirect Coombs test); b) expanding the obstetric history, focusing on sensitizing events; and c) providing parental counseling about potential risks and additional tests.\\nAfter a sensitizing event, it is recommended to administer anti-D IgG within the first 72 hours at a dose of 1500 IU (300 μg). If not feasible, it can be administered up to 4 weeks after the event if it was not given initially.\\n\\n7.1. For non-isoimmunized pregnant women (with a negative Coombs test and Rh-positive newborn), it is recommended to administer anti-D IgG between weeks 28 and 32, and within the first 72 hours postpartum if the newborn is Rh-positive. The dose is 300 μg IM or IV.\\n\\n7.2. In the case of a cesarean section in an Rh-D negative patient with a Rh-D positive child, the consensus does not recommend doubling the dose of anti-D IgG. The dose remains the same as after a vaginal delivery: 300 μg IM or IV.\\n\\n7.3. In a twin delivery involving an Rh-D negative patient with two or more Rh-D positive live-born infants, the consensus recommends not doubling the dose of anti-D IgG. The dose remains 300 μg IM or IV, the same as after a vaginal delivery.\\n\\n7.4. For a non-isoimmunized Rh-D negative patient in the puerperium with immediate postpartum surgical tubal sterilization and an Rh-D positive neonate, anti-D IgG is recommended, assuming no prior sensitization, given the potential for reproductive decision changes or failure of the procedure.\\n\\nAn Rh-D negative patient is considered isoimmunized if: a) the indirect Coombs test is positive at any titer, provided anti-D IgG was not received in the previous month, or b) there is a history of adverse perinatal outcomes associated with Rh disease in prior pregnancies, such as hydrops.\\n9.1. If Rh-D negative women are isoimmunized, it is necessary to determine the anti-D antibody titer, as this titer correlates with the severity of the disease and determines the need for fetal anemia studies with Doppler velocimetry of the MCA.\\n\\n9.2. For isoimmunized Rh-D negative patients, it is recommended to follow up with monthly quantitative indirect Coombs tests until week 24, then bi-weekly, or until reaching a critical titer (≥ 1:16).\\n\\n10.1. Doppler ultrasound of the MCA is suggested for Rh-D negative patients with a positive indirect Coombs test and titers ≥ 1:16.\\n\\n10.2. In non-isoimmunized Rh-D negative patients, the consensus does not recommend MCA Doppler velocimetry.\\n\\n10.3. Weekly MCA Doppler ultrasounds are recommended for isoimmunized patients with indirect Coombs titers ≥ 1:16.\\n\\n10.4. The consensus suggests adopting a cut-off value of ≥ 1.5 multiples of the median (MoM) of the peak systolic velocity for gestational age on MCA Doppler, as this value best correlates with fetal anemia.\\n\\nThe consensus suggests Cordocentesis when fetal anemia is suspected, and intrauterine fetal transfusion when cordocentesis shows severe fetal anemia. This procedure should be performed by trained personnel.\\nIt is recommended to prolong pregnancy until the fetus has achieved sufficient lung and tissue maturation to improve perinatal survival, according to the indirect Coombs test titer threshold.</p><p><strong>Conclusions: </strong>It is essential to address Rh-D negative pregnant women, isoimmunized women, and fetuses with Rh disease in an appropriate and standardized manner, according to the Colombian context, across all levels of prenatal care. The recommendations issued in this consensus are expected to improve clinical care, as well as enhance perinatal health and neonatal quality of life in cases of Rh disease.</p>\",\"PeriodicalId\":101422,\"journal\":{\"name\":\"Revista colombiana de obstetricia y ginecologia\",\"volume\":\"75 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11457932/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Revista colombiana de obstetricia y ginecologia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18597/rcog.4142\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista colombiana de obstetricia y ginecologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18597/rcog.4142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
[Colombian consensus for the diagnosis, prevention, and management of Rhesus disease].
Objective: To train healthcare professionals involved in the care of Rh-D negative pregnant women, with the aim of standardizing the management of Rh isoimmunization prevention, timely antenatal diagnosis of Rh disease, fetal assessment, and treatment of fetuses with Rh disease, in order to prevent adverse perinatal outcomes.
Materials and methods: A group of 23 expert panelists participated in the development of the consensus through three rounds, answering a questionnaire consisting of 8 domains and 22 questions. A modified Delphi method was used until the consensus threshold among participants was reached, defined as 80% or greater agreement in responses. In the third round of the expert panel, a twenty-third question emerged, which was answered by one of the thematic leaders. The eight domains of antenatal management for Rh-D negative pregnant women were: 1) Rh-D determination, 2) initial prenatal care for Rh-D negative patients, 3) titration and periodicity of the indirect Coombs test, 4) sensitizing events, 5) administration of anti-D immunoglobulin (IgG), 6) Doppler velocimetry of the middle cerebral artery (MCA), 7) antenatal management of isoimmunized patients and anemic fetuses, and 8) timing for pregnancy termination based on different clinical scenarios. Based on these responses, and a review of international clinical practice guidelines, consensus statements were formulated, including recommendations, their justification, and adaptation to the local context.
Results: The following recommendations were issued:
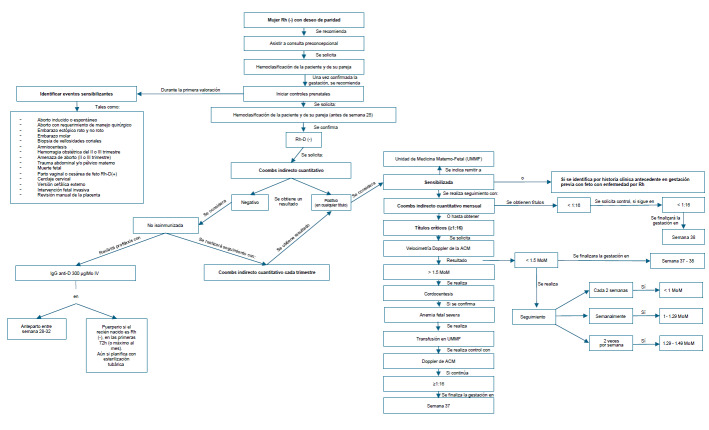
It is suggested that Rh-D negative women of childbearing age attend a preconception consultation.
It is recommended to determine maternal Rh-D status at the first contact with health services, either during the preconception consultation or at the first prenatal check-up.
For Rh-D negative patients, it is recommended to determine the Rh-D status of the child's father during prenatal care as early as possible, preferably before the 28th week of gestation.
For Rh-D negative primigravidas, where the father is Rh-D positive, it is suggested to: a) determine and quantify Rh-D antibodies (indirect Coombs test) during the first consultation and then quarterly, b) expand the obstetric history, with an emphasis on identifying sensitizing events, and c) provide parental counseling regarding potential risks, the need for additional tests, and the possibility of immunization during pregnancy.
During prenatal care for Rh-D negative multiparous patients with previous Rh-D positive offspring, the initial approach should include: a) determining and titrating Rh-D antibodies (indirect Coombs test); b) expanding the obstetric history, focusing on sensitizing events; and c) providing parental counseling about potential risks and additional tests.
After a sensitizing event, it is recommended to administer anti-D IgG within the first 72 hours at a dose of 1500 IU (300 μg). If not feasible, it can be administered up to 4 weeks after the event if it was not given initially.
7.1. For non-isoimmunized pregnant women (with a negative Coombs test and Rh-positive newborn), it is recommended to administer anti-D IgG between weeks 28 and 32, and within the first 72 hours postpartum if the newborn is Rh-positive. The dose is 300 μg IM or IV.
7.2. In the case of a cesarean section in an Rh-D negative patient with a Rh-D positive child, the consensus does not recommend doubling the dose of anti-D IgG. The dose remains the same as after a vaginal delivery: 300 μg IM or IV.
7.3. In a twin delivery involving an Rh-D negative patient with two or more Rh-D positive live-born infants, the consensus recommends not doubling the dose of anti-D IgG. The dose remains 300 μg IM or IV, the same as after a vaginal delivery.
7.4. For a non-isoimmunized Rh-D negative patient in the puerperium with immediate postpartum surgical tubal sterilization and an Rh-D positive neonate, anti-D IgG is recommended, assuming no prior sensitization, given the potential for reproductive decision changes or failure of the procedure.
An Rh-D negative patient is considered isoimmunized if: a) the indirect Coombs test is positive at any titer, provided anti-D IgG was not received in the previous month, or b) there is a history of adverse perinatal outcomes associated with Rh disease in prior pregnancies, such as hydrops.
9.1. If Rh-D negative women are isoimmunized, it is necessary to determine the anti-D antibody titer, as this titer correlates with the severity of the disease and determines the need for fetal anemia studies with Doppler velocimetry of the MCA.
9.2. For isoimmunized Rh-D negative patients, it is recommended to follow up with monthly quantitative indirect Coombs tests until week 24, then bi-weekly, or until reaching a critical titer (≥ 1:16).
10.1. Doppler ultrasound of the MCA is suggested for Rh-D negative patients with a positive indirect Coombs test and titers ≥ 1:16.
10.2. In non-isoimmunized Rh-D negative patients, the consensus does not recommend MCA Doppler velocimetry.
10.3. Weekly MCA Doppler ultrasounds are recommended for isoimmunized patients with indirect Coombs titers ≥ 1:16.
10.4. The consensus suggests adopting a cut-off value of ≥ 1.5 multiples of the median (MoM) of the peak systolic velocity for gestational age on MCA Doppler, as this value best correlates with fetal anemia.
The consensus suggests Cordocentesis when fetal anemia is suspected, and intrauterine fetal transfusion when cordocentesis shows severe fetal anemia. This procedure should be performed by trained personnel.
It is recommended to prolong pregnancy until the fetus has achieved sufficient lung and tissue maturation to improve perinatal survival, according to the indirect Coombs test titer threshold.
Conclusions: It is essential to address Rh-D negative pregnant women, isoimmunized women, and fetuses with Rh disease in an appropriate and standardized manner, according to the Colombian context, across all levels of prenatal care. The recommendations issued in this consensus are expected to improve clinical care, as well as enhance perinatal health and neonatal quality of life in cases of Rh disease.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
