Elias K. Mai, Axel Nogai, Henk M. Lokhorst, Bronno van der Holt, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Anna Jauch, Jens Hillengass, Marian Stevens-Kroef, Marc S. Raab, Annemiek Broijl, Gerard M. J. Bos, Peter Brossart, Paula Ypma, Christine Hanoun, Uta Bertsch, Thomas Hielscher, Hans J. Salwender, Christoph Scheid, Hartmut Goldschmidt, Pieter Sonneveld
{"title":"对符合移植条件的新诊断多发性骨髓瘤患者进行大剂量治疗前后的硼替佐米治疗:HOVON-65/GMMG-HD4 III期试验10多年随访后的长期总生存率","authors":"Elias K. Mai, Axel Nogai, Henk M. Lokhorst, Bronno van der Holt, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Anna Jauch, Jens Hillengass, Marian Stevens-Kroef, Marc S. Raab, Annemiek Broijl, Gerard M. J. Bos, Peter Brossart, Paula Ypma, Christine Hanoun, Uta Bertsch, Thomas Hielscher, Hans J. Salwender, Christoph Scheid, Hartmut Goldschmidt, Pieter Sonneveld","doi":"10.1002/hem3.70052","DOIUrl":null,"url":null,"abstract":"<p>Life expectancy in patients with multiple myeloma (MM) has increased due to the availability of effective drugs such as proteasome inhibitors (PIs),<span><sup>1, 2</sup></span> immunomodulatory drugs (IMiDs),<span><sup>3-5</sup></span> and more recently, monoclonal antibodies.<span><sup>6-8</sup></span></p><p>While the progression-free survival (PFS) rates and the depth of response increase with the use of modern multi-drug combinations, it is not clear whether these effects will translate into an improved long-term overall survival (OS). To draw such conclusions, long-term follow-up analyses from trials are needed as comparators for future trials. Here, we report on the long-term overall survival of the HOVON-65/GMMG-HD4 trial including the OS after more than 10 years, and the role of established prognostic factors.</p><p>The investigator-sponsored, open-label, randomized HOVON-65/GMMG-HD4 phase III trial was conducted by the Dutch-Belgian Cooperative Trial Group for Hematology Oncology (HOVON) and the German-speaking Myeloma Multicenter Group (GMMG) in 75 centers in the Netherlands, Belgium, and Germany from May 2005 to May 2008 and included 827 eligible patients. The trial was registered at www.trialregister.nl (until June 2022) and https://trialsearch.who.int/ as NTR213, at www.isrctn.com as ISRCTN64455289 and at www.clinicaltrialsregister.eu as EudraCT2004-000944-26. The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).</p><p>Initial results of the trial have been published and include a detailed study protocol, inclusion and exclusion criteria, randomization procedures and toxicities,<span><sup>9</sup></span> and results after a median follow-up of 96 months.<span><sup>10</sup></span> After that, only OS data were collected on which we here report the final long-term survival data.</p><p>The aim of the trial was to investigate the use of bortezomib (BTZ) in induction and maintenance compared to treatment with classical cytotoxic agents as induction and thalidomide maintenance in transplant-eligible patients regarding the primary endpoint PFS, while OS was a secondary endpoint. Patients were randomized 1:1 to receive either vincristine, adriamycin, and dexamethasone (VAD) as induction therapy, followed by high-dose chemotherapy with melphalan and autologous stem-cell transplantation (ASCT), followed by maintenance therapy with thalidomide (VAD arm). In the PAD arm, BTZ, adriamycin, and dexamethasone were used in induction, followed by ASCT and maintenance with BTZ. Patients were stratified by center and International Staging System (ISS, I vs. II vs. III). A single ASCT was planned in the HOVON group, whereas in the GMMG, a tandem ASCT was planned. Patients with an HLA-identical sibling could proceed to allogeneic stem cell transplantation (alloSCT) after the first ASCT.</p><p>For the current exploratory analysis, the data available at the final database lock were used (as of July 4, 2019). OS was calculated from randomization until death from any cause, censoring patients alive at the date of last contact.<span><sup>9</sup></span> OS was estimated by the Kaplan–Meier method, and 95% confidence intervals (CIs) were constructed. The formal test for difference in OS between the two treatment arms was done with a Cox regression analysis with adjustment for the stratification factor ISS. HRs and corresponding 95% CIs were determined. Kaplan–Meier curves were generated to illustrate survival. All analyses were performed on the intention-to-treat population. All reported <i>p</i>-values are two-sided and have not been adjusted for multiple testing. A detailed summary of the trial, eligibility criteria, treatment, response assessment, endpoints, and statistical analysis can be found in the Supporting Information Appendix (pages 3–5) and has been published previously.<span><sup>9, 10</sup></span></p><p>From May 2005 to May 2008, 833 patients were randomly assigned 1:1 to the treatment arms, with 413 and 414 eligible patients being randomized to the VAD and PAD arm, respectively. Six patients were ineligible and excluded from all analyses. Baseline characteristics were reported previously and were evenly distributed.<span><sup>9</sup></span></p><p>Since July 2011, all patients are in follow-up. Differences in the applied treatments between the HOVON and GMMG study groups have been described before.<span><sup>9, 10</sup></span> In short, in the HOVON group, the number of patients receiving an allogeneic stem cell transplantation was higher (HOVON 60 patients vs. GMMG 2 patients), while in the GMMG study group, more patients received an upfront tandem ASCT (GMMG 273 patients; HOVON 2 patients). Maintenance therapy according to the protocol was initiated in 217 patients in the HOVON group and in 283 patients in the GMMG group with a longer duration of study in the GMMG group.<span><sup>10</sup></span> A consort diagram for each study group (HOVON and GMMG) and data on documented systemic treatment after the first relapse/progression for MM have been reported previously.<span><sup>10</sup></span></p><p>Of the 827 patients, 508 (61%) have died and 78 (9%) patients were lost to follow-up. The median follow-up of the 319 patients still alive including the patients lost to follow-up is 11.4 years (inter-quartile range: 10.2–12.3). The 12-year OS in the VAD arm was 32% (95% CI: 27%–37%) versus 36% (95% CI: 31%–41%) in the PAD arm (Figure 1A and Supporting Information Appendix page 6). The difference in OS was not statistically significant, neither in the Cox regression analysis (HR = 0.87, 95% CI: 0.73–1.04, <i>p</i> = 0.12, adjusted for ISS) nor with the stratified log-rank test (<i>p</i> = 0.15). Univariable analyses are shown as forest plots in Figure 1B. As in the previous reports,<span><sup>9, 10</sup></span> patient subgroups with ISS stage 3 (HR = 0.66, 95% CI: 0.45–0.97), del(13q14) (HR = 0.68, 95% CI: 0.51–0.90), and renal impairment (HR = 0.31, 95% CI: 0.16–0.57) showed a promising benefit from PAD versus VAD treatment. To further assess the prognostic value of selected baseline characteristics on OS, multivariable Cox regression analysis was performed (Table 1). This analysis revealed a statistically significant OS benefit in favor of the PAD versus VAD arm (HR = 0.84, 95% CI: 0.70–1.00, <i>p</i> = 0.048).</p><p>OS on patients with renal impairment, adverse cytogenetics (GMMG patients only<span><sup>10</sup></span>), and according to response status as previously analyzed are shown in Supporting Information S1: Figures 1–3 and remained unchanged with regard to the previous long-term follow-up of the trial.<span><sup>10</sup></span> In this trial, the use of single versus tandem ASCT was not determined as per the study protocol. However, the procedures between the study groups differed especially regarding upfront allogeneic transplantation, the use of tandem ASCT, and the duration of maintenance therapy.<span><sup>10</sup></span> A post hoc analysis of OS from the date of the last ASCT showed a 10-year OS for 41% (95% CI: 36%–45%) of patients after single, and 41% (95% CI: 34%–47%) of patients after tandem ASCT (HR = 0.99, 95% CI: 0.81–1.21, <i>p</i> = 0.93).</p><p>In this final long-term follow-up of the multicenter, phase III trial HOVON-65/GMMG-HD4 with a median follow-up of 11.4 years, more than 35% of patients are alive, and 10-year OS of the overall intention-to-treat population is 40% (95% CI: 36%–43%). OS did not differ significantly between the study arms in univariable analyses but showed a significant OS advantage for the PAD arm in a multivariable analysis. Treatment in the PAD arm led to improved PFS as was already shown in the previous analyses.<span><sup>9, 10</sup></span> In patients with renal impairment, OS improved significantly with PAD compared to VAD, resulting in a similar OS as compared to patients without renal impairment. Similarly, the negative prognostic impact of del(17p13) was overcome in the PAD arm with a remarkable 37% OS at 10 years compared to 43% in patients without del(17p13).</p><p>Whether the use of a tandem ASCT improves the outcome was extensively elaborated and discussed in an earlier analysis of this study.<span><sup>10</sup></span> Because of the described confounders it is not possible to draw a definite conclusion about the efficacy of a tandem ASCT compared to a single ASCT from this trial.</p><p>Despite comparing chemotherapy plus thalidomide-based to a bortezomib-based strategy, the difference regarding OS is rather small. Likely, a less effective therapy during the first line might be partially overcome by the use of novel therapies in relapsed MM. Bortezomib was indeed used in a higher number of patients at first relapse in the VAD as compared to the PAD arm (60% vs. 33%).<span><sup>10</sup></span> Several novel agents have been developed for MM treatment after the completion of this trial.<span><sup>2, 6, 7</sup></span> Therefore, patients with a longer PFS after first-line treatment may have been more likely to be treated with these novel agents after relapse than patients with an early relapse. Since patients with early relapse are usually patients with high-risk features, and the fact that at the time of relapse these novel, more effective agents may not have been available yet, this may in part explain our OS results, particularly in high-risk MM, and support risk-adapted strategies with more intense induction therapies for patients with high-risk features.<span><sup>11</sup></span> Yet, long-term OS as an outcome measure remains important to elucidate differences in therapeutic strategies.</p><p>In summary, in this final long-term follow-up analysis, the primary analysis did not show a statistically significant improvement in OS. However, improvement of OS in subgroups of patients with a del(17p13) or renal impairment was observed. Furthermore, the survival of a substantial fraction of patients for 12 years and longer indicates the effectiveness of current treatment strategies for MM and underlines the importance of long-term follow-up analysis in future trials.</p><p>Pieter Sonneveld, Peter Brossart, Sonja Zweegman, Gerard M. J. Bos, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in conception and design. Bronno van der Holt, Uta Bertsch, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in administrative support. Pieter Sonneveld, Hans J. Salwender, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Jens Hillengass, Marc S. Raab, Christine Hanoun, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in provision of study materials or patients. Pieter Sonneveld, Peter Brossart, Uta Bertsch, Hans J. Salwender, Sonja Zweegman, Annemiek Broijl, Axel Nogai, Katja C. Weisel, Jens Hillengass, Marc S. Raab, Elias K. Mai, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Anna Jauch, Thomas Hielscher, Christine Hanoun, Paula Ypma, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in collection and assembly of data. Elias K. Mai, Axel Nogai, Bronno van der Holt, Sonja Zweegman, Marian Stevens-Kroef, Christoph Scheid, Paula Ypma, Thomas Hielscher, Hartmut Goldschmidt, and Pieter Sonneveld were involved in data analysis and interpretation. Elias K. Mai, Axel Nogai, and Bronno van der Holt were involved in writing of the first manuscript draft. All authors involved in manuscript editing and writing, final approval of manuscript.</p><p>Elias K. Mai reports consulting or advisory role with Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; honoraria from Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; research funding from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, and Takeda; and travel accommodations and expenses from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, Stemline, and Takeda. Axel Nogai reports consulting or advisory role with Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi and GSK; honoraria from Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi, and GSK; research support from BMS, Janssen, and Celgene; and travel accommodations and expenses from Takeda, Janssen, Alexion, and Amgen. Bronno van der Holt reports honoraria for data safety monitoring board membership from IFM. Sonja Zweegman reports consulting or advisory role with Janssen, BMS, Sanofi, Oncopeptides, and GSK; and research funding from Takeda and Janssen. Katja C. Weisel reports consulting or advisory role with Abbvie, Amgen, Adaptive Biotech, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Oncopeptides, Pfizer, Regeneron, Roche Pharma, Sanofi, Takeda, and Menarini; honoraria from Abbvie, Amgen, Adaptive Biotech, Astra Zeneca, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Novartis, Oncopeptides, Pfizer, Roche Pharma, Sanofi, Stemline, Takeda, and Menarini; and research funding from Abbvie, Amgen, Bristol Myers Squibb/Celgene, Janssen, GlaxoSmithKline, Pfizer, Sanofi, and Takeda. Jens Hillengass reports advisory role with Prothena, Sebia, and Regeneron; honoraria from Targeted Oncology; and member of data safety monitoring boards with Janssen. Marc S. Raab reports consulting or advisory role with BMS, Amgen, GSK, Janssen, Sanofi, Pfizer, AbbVie, and Takeda; research funding from BMS, Janssen, Sanofi, and Heidelberg Pharma; travel accommodation and expenses from BMS, Amgen, and Janssen; and honoraria from BMS, Janssen, AbbVie, and Sanofi. Annemiek Broijl reports honoraria from Amgen, Sanofi, Janssen, and BMS. Peter Brossart reports consulting or advisory role from Astra-Zeneca, BMS, MSD, BeiGene, and Gilead; research funding from BMS; and honoraria from Gilead, MSD, BMS, and Astra-Zeneca. Christoph Scheid reports consulting or advisory role from Bristol Myers Squibb, GlaxoSmithKline, Janssen, Pfizer, Roche, and Takeda; honoraria from Amgen, Bristol Myers Squibb, GlaxoSmithKline, Janssen, MSD, Novartis, Roche, Sanofi, and Takeda; research funding from Janssen, and Takeda; and travel accommodation and expenses from Bristol Myers Squibb, Janssen, Sanofi Aventis, and Takeda. Hans J. Salwender reports consulting or advisory role with Amgen, AstraZeneca, Bristol Myers Squibb/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Sanofi, and Stemline; honoraria from Abbvie, Amgen, AstraZeneca, Bristol Myers SquibbMS/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Roche, Sanofi, Stemline, and Takeda; and travel accommodation and expenses from Amgen, Bristol Myers Squibb/Celgene, Janssen Cilag, and Sanofi. Hartmut Goldschmidt reports consulting or advisory role with Amgen, BMS, Janssen, Sanofi, and Adaptive Biotechnology; honoraria from Amgen, BMS, Chugai, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; research funding from Amgen, BMS, Celgene, GlycoMimetics Inc., GlaxoSmithKline, Heidelberg Pharma, Hoffmann-La Roche, Karyopharm, Janssen, Incyte Corporation, Millenium Pharmaceuticals Inc., Molecular Partners, Merck Sharp and Dohme, MorphoSys AG, Pfizer, Sanofi, Takeda, and Novartis; travel accommodations and expenses from Amgen, BMS, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; grants from Amgen, Array Biopharma/Pfizer, BMS/Celgene, Chugai, Dietmar-Hopp-Foundation, Janssen, Johns Hopkins University, Mundipharma GmbH, and Sanofi. Pieter Sonneveld reports advisory role with Amgen, BMS, Celgene, Janssen, Karyopharm, and Pfizer; research funding from Amgen, BMS, Janssen, and Karyopharm. All other authors declare no competing interests.</p><p>The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).</p><p>The HOVON-65/GMMG-HD4 trial was supported by the Dutch Cancer Foundation, the German Federal Ministry of Education and Research, and unrestricted Grant No. MMY3003 from Janssen-Cilag-Ortho Biotech. The German-speaking Myeloma Multicenter Group was supported by grants from Novartis, Amgen (No. P2004-0060), Chugai, and Roche.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"8 11","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2024-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70052","citationCount":"0","resultStr":"{\"title\":\"Bortezomib before and after high-dose therapy in transplant-eligible patients with newly diagnosed multiple myeloma: Long-term overall survival after more than 10 years of follow-up from the phase III HOVON-65/GMMG-HD4 trial\",\"authors\":\"Elias K. Mai, Axel Nogai, Henk M. Lokhorst, Bronno van der Holt, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Anna Jauch, Jens Hillengass, Marian Stevens-Kroef, Marc S. Raab, Annemiek Broijl, Gerard M. J. Bos, Peter Brossart, Paula Ypma, Christine Hanoun, Uta Bertsch, Thomas Hielscher, Hans J. Salwender, Christoph Scheid, Hartmut Goldschmidt, Pieter Sonneveld\",\"doi\":\"10.1002/hem3.70052\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Life expectancy in patients with multiple myeloma (MM) has increased due to the availability of effective drugs such as proteasome inhibitors (PIs),<span><sup>1, 2</sup></span> immunomodulatory drugs (IMiDs),<span><sup>3-5</sup></span> and more recently, monoclonal antibodies.<span><sup>6-8</sup></span></p><p>While the progression-free survival (PFS) rates and the depth of response increase with the use of modern multi-drug combinations, it is not clear whether these effects will translate into an improved long-term overall survival (OS). To draw such conclusions, long-term follow-up analyses from trials are needed as comparators for future trials. Here, we report on the long-term overall survival of the HOVON-65/GMMG-HD4 trial including the OS after more than 10 years, and the role of established prognostic factors.</p><p>The investigator-sponsored, open-label, randomized HOVON-65/GMMG-HD4 phase III trial was conducted by the Dutch-Belgian Cooperative Trial Group for Hematology Oncology (HOVON) and the German-speaking Myeloma Multicenter Group (GMMG) in 75 centers in the Netherlands, Belgium, and Germany from May 2005 to May 2008 and included 827 eligible patients. The trial was registered at www.trialregister.nl (until June 2022) and https://trialsearch.who.int/ as NTR213, at www.isrctn.com as ISRCTN64455289 and at www.clinicaltrialsregister.eu as EudraCT2004-000944-26. The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).</p><p>Initial results of the trial have been published and include a detailed study protocol, inclusion and exclusion criteria, randomization procedures and toxicities,<span><sup>9</sup></span> and results after a median follow-up of 96 months.<span><sup>10</sup></span> After that, only OS data were collected on which we here report the final long-term survival data.</p><p>The aim of the trial was to investigate the use of bortezomib (BTZ) in induction and maintenance compared to treatment with classical cytotoxic agents as induction and thalidomide maintenance in transplant-eligible patients regarding the primary endpoint PFS, while OS was a secondary endpoint. Patients were randomized 1:1 to receive either vincristine, adriamycin, and dexamethasone (VAD) as induction therapy, followed by high-dose chemotherapy with melphalan and autologous stem-cell transplantation (ASCT), followed by maintenance therapy with thalidomide (VAD arm). In the PAD arm, BTZ, adriamycin, and dexamethasone were used in induction, followed by ASCT and maintenance with BTZ. Patients were stratified by center and International Staging System (ISS, I vs. II vs. III). A single ASCT was planned in the HOVON group, whereas in the GMMG, a tandem ASCT was planned. Patients with an HLA-identical sibling could proceed to allogeneic stem cell transplantation (alloSCT) after the first ASCT.</p><p>For the current exploratory analysis, the data available at the final database lock were used (as of July 4, 2019). OS was calculated from randomization until death from any cause, censoring patients alive at the date of last contact.<span><sup>9</sup></span> OS was estimated by the Kaplan–Meier method, and 95% confidence intervals (CIs) were constructed. The formal test for difference in OS between the two treatment arms was done with a Cox regression analysis with adjustment for the stratification factor ISS. HRs and corresponding 95% CIs were determined. Kaplan–Meier curves were generated to illustrate survival. All analyses were performed on the intention-to-treat population. All reported <i>p</i>-values are two-sided and have not been adjusted for multiple testing. A detailed summary of the trial, eligibility criteria, treatment, response assessment, endpoints, and statistical analysis can be found in the Supporting Information Appendix (pages 3–5) and has been published previously.<span><sup>9, 10</sup></span></p><p>From May 2005 to May 2008, 833 patients were randomly assigned 1:1 to the treatment arms, with 413 and 414 eligible patients being randomized to the VAD and PAD arm, respectively. Six patients were ineligible and excluded from all analyses. Baseline characteristics were reported previously and were evenly distributed.<span><sup>9</sup></span></p><p>Since July 2011, all patients are in follow-up. Differences in the applied treatments between the HOVON and GMMG study groups have been described before.<span><sup>9, 10</sup></span> In short, in the HOVON group, the number of patients receiving an allogeneic stem cell transplantation was higher (HOVON 60 patients vs. GMMG 2 patients), while in the GMMG study group, more patients received an upfront tandem ASCT (GMMG 273 patients; HOVON 2 patients). Maintenance therapy according to the protocol was initiated in 217 patients in the HOVON group and in 283 patients in the GMMG group with a longer duration of study in the GMMG group.<span><sup>10</sup></span> A consort diagram for each study group (HOVON and GMMG) and data on documented systemic treatment after the first relapse/progression for MM have been reported previously.<span><sup>10</sup></span></p><p>Of the 827 patients, 508 (61%) have died and 78 (9%) patients were lost to follow-up. The median follow-up of the 319 patients still alive including the patients lost to follow-up is 11.4 years (inter-quartile range: 10.2–12.3). The 12-year OS in the VAD arm was 32% (95% CI: 27%–37%) versus 36% (95% CI: 31%–41%) in the PAD arm (Figure 1A and Supporting Information Appendix page 6). The difference in OS was not statistically significant, neither in the Cox regression analysis (HR = 0.87, 95% CI: 0.73–1.04, <i>p</i> = 0.12, adjusted for ISS) nor with the stratified log-rank test (<i>p</i> = 0.15). Univariable analyses are shown as forest plots in Figure 1B. As in the previous reports,<span><sup>9, 10</sup></span> patient subgroups with ISS stage 3 (HR = 0.66, 95% CI: 0.45–0.97), del(13q14) (HR = 0.68, 95% CI: 0.51–0.90), and renal impairment (HR = 0.31, 95% CI: 0.16–0.57) showed a promising benefit from PAD versus VAD treatment. To further assess the prognostic value of selected baseline characteristics on OS, multivariable Cox regression analysis was performed (Table 1). This analysis revealed a statistically significant OS benefit in favor of the PAD versus VAD arm (HR = 0.84, 95% CI: 0.70–1.00, <i>p</i> = 0.048).</p><p>OS on patients with renal impairment, adverse cytogenetics (GMMG patients only<span><sup>10</sup></span>), and according to response status as previously analyzed are shown in Supporting Information S1: Figures 1–3 and remained unchanged with regard to the previous long-term follow-up of the trial.<span><sup>10</sup></span> In this trial, the use of single versus tandem ASCT was not determined as per the study protocol. However, the procedures between the study groups differed especially regarding upfront allogeneic transplantation, the use of tandem ASCT, and the duration of maintenance therapy.<span><sup>10</sup></span> A post hoc analysis of OS from the date of the last ASCT showed a 10-year OS for 41% (95% CI: 36%–45%) of patients after single, and 41% (95% CI: 34%–47%) of patients after tandem ASCT (HR = 0.99, 95% CI: 0.81–1.21, <i>p</i> = 0.93).</p><p>In this final long-term follow-up of the multicenter, phase III trial HOVON-65/GMMG-HD4 with a median follow-up of 11.4 years, more than 35% of patients are alive, and 10-year OS of the overall intention-to-treat population is 40% (95% CI: 36%–43%). OS did not differ significantly between the study arms in univariable analyses but showed a significant OS advantage for the PAD arm in a multivariable analysis. Treatment in the PAD arm led to improved PFS as was already shown in the previous analyses.<span><sup>9, 10</sup></span> In patients with renal impairment, OS improved significantly with PAD compared to VAD, resulting in a similar OS as compared to patients without renal impairment. Similarly, the negative prognostic impact of del(17p13) was overcome in the PAD arm with a remarkable 37% OS at 10 years compared to 43% in patients without del(17p13).</p><p>Whether the use of a tandem ASCT improves the outcome was extensively elaborated and discussed in an earlier analysis of this study.<span><sup>10</sup></span> Because of the described confounders it is not possible to draw a definite conclusion about the efficacy of a tandem ASCT compared to a single ASCT from this trial.</p><p>Despite comparing chemotherapy plus thalidomide-based to a bortezomib-based strategy, the difference regarding OS is rather small. Likely, a less effective therapy during the first line might be partially overcome by the use of novel therapies in relapsed MM. Bortezomib was indeed used in a higher number of patients at first relapse in the VAD as compared to the PAD arm (60% vs. 33%).<span><sup>10</sup></span> Several novel agents have been developed for MM treatment after the completion of this trial.<span><sup>2, 6, 7</sup></span> Therefore, patients with a longer PFS after first-line treatment may have been more likely to be treated with these novel agents after relapse than patients with an early relapse. Since patients with early relapse are usually patients with high-risk features, and the fact that at the time of relapse these novel, more effective agents may not have been available yet, this may in part explain our OS results, particularly in high-risk MM, and support risk-adapted strategies with more intense induction therapies for patients with high-risk features.<span><sup>11</sup></span> Yet, long-term OS as an outcome measure remains important to elucidate differences in therapeutic strategies.</p><p>In summary, in this final long-term follow-up analysis, the primary analysis did not show a statistically significant improvement in OS. However, improvement of OS in subgroups of patients with a del(17p13) or renal impairment was observed. Furthermore, the survival of a substantial fraction of patients for 12 years and longer indicates the effectiveness of current treatment strategies for MM and underlines the importance of long-term follow-up analysis in future trials.</p><p>Pieter Sonneveld, Peter Brossart, Sonja Zweegman, Gerard M. J. Bos, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in conception and design. Bronno van der Holt, Uta Bertsch, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in administrative support. Pieter Sonneveld, Hans J. Salwender, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Jens Hillengass, Marc S. Raab, Christine Hanoun, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in provision of study materials or patients. Pieter Sonneveld, Peter Brossart, Uta Bertsch, Hans J. Salwender, Sonja Zweegman, Annemiek Broijl, Axel Nogai, Katja C. Weisel, Jens Hillengass, Marc S. Raab, Elias K. Mai, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Anna Jauch, Thomas Hielscher, Christine Hanoun, Paula Ypma, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in collection and assembly of data. Elias K. Mai, Axel Nogai, Bronno van der Holt, Sonja Zweegman, Marian Stevens-Kroef, Christoph Scheid, Paula Ypma, Thomas Hielscher, Hartmut Goldschmidt, and Pieter Sonneveld were involved in data analysis and interpretation. Elias K. Mai, Axel Nogai, and Bronno van der Holt were involved in writing of the first manuscript draft. All authors involved in manuscript editing and writing, final approval of manuscript.</p><p>Elias K. Mai reports consulting or advisory role with Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; honoraria from Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; research funding from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, and Takeda; and travel accommodations and expenses from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, Stemline, and Takeda. Axel Nogai reports consulting or advisory role with Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi and GSK; honoraria from Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi, and GSK; research support from BMS, Janssen, and Celgene; and travel accommodations and expenses from Takeda, Janssen, Alexion, and Amgen. Bronno van der Holt reports honoraria for data safety monitoring board membership from IFM. Sonja Zweegman reports consulting or advisory role with Janssen, BMS, Sanofi, Oncopeptides, and GSK; and research funding from Takeda and Janssen. Katja C. Weisel reports consulting or advisory role with Abbvie, Amgen, Adaptive Biotech, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Oncopeptides, Pfizer, Regeneron, Roche Pharma, Sanofi, Takeda, and Menarini; honoraria from Abbvie, Amgen, Adaptive Biotech, Astra Zeneca, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Novartis, Oncopeptides, Pfizer, Roche Pharma, Sanofi, Stemline, Takeda, and Menarini; and research funding from Abbvie, Amgen, Bristol Myers Squibb/Celgene, Janssen, GlaxoSmithKline, Pfizer, Sanofi, and Takeda. Jens Hillengass reports advisory role with Prothena, Sebia, and Regeneron; honoraria from Targeted Oncology; and member of data safety monitoring boards with Janssen. Marc S. Raab reports consulting or advisory role with BMS, Amgen, GSK, Janssen, Sanofi, Pfizer, AbbVie, and Takeda; research funding from BMS, Janssen, Sanofi, and Heidelberg Pharma; travel accommodation and expenses from BMS, Amgen, and Janssen; and honoraria from BMS, Janssen, AbbVie, and Sanofi. Annemiek Broijl reports honoraria from Amgen, Sanofi, Janssen, and BMS. Peter Brossart reports consulting or advisory role from Astra-Zeneca, BMS, MSD, BeiGene, and Gilead; research funding from BMS; and honoraria from Gilead, MSD, BMS, and Astra-Zeneca. Christoph Scheid reports consulting or advisory role from Bristol Myers Squibb, GlaxoSmithKline, Janssen, Pfizer, Roche, and Takeda; honoraria from Amgen, Bristol Myers Squibb, GlaxoSmithKline, Janssen, MSD, Novartis, Roche, Sanofi, and Takeda; research funding from Janssen, and Takeda; and travel accommodation and expenses from Bristol Myers Squibb, Janssen, Sanofi Aventis, and Takeda. Hans J. Salwender reports consulting or advisory role with Amgen, AstraZeneca, Bristol Myers Squibb/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Sanofi, and Stemline; honoraria from Abbvie, Amgen, AstraZeneca, Bristol Myers SquibbMS/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Roche, Sanofi, Stemline, and Takeda; and travel accommodation and expenses from Amgen, Bristol Myers Squibb/Celgene, Janssen Cilag, and Sanofi. Hartmut Goldschmidt reports consulting or advisory role with Amgen, BMS, Janssen, Sanofi, and Adaptive Biotechnology; honoraria from Amgen, BMS, Chugai, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; research funding from Amgen, BMS, Celgene, GlycoMimetics Inc., GlaxoSmithKline, Heidelberg Pharma, Hoffmann-La Roche, Karyopharm, Janssen, Incyte Corporation, Millenium Pharmaceuticals Inc., Molecular Partners, Merck Sharp and Dohme, MorphoSys AG, Pfizer, Sanofi, Takeda, and Novartis; travel accommodations and expenses from Amgen, BMS, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; grants from Amgen, Array Biopharma/Pfizer, BMS/Celgene, Chugai, Dietmar-Hopp-Foundation, Janssen, Johns Hopkins University, Mundipharma GmbH, and Sanofi. Pieter Sonneveld reports advisory role with Amgen, BMS, Celgene, Janssen, Karyopharm, and Pfizer; research funding from Amgen, BMS, Janssen, and Karyopharm. All other authors declare no competing interests.</p><p>The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).</p><p>The HOVON-65/GMMG-HD4 trial was supported by the Dutch Cancer Foundation, the German Federal Ministry of Education and Research, and unrestricted Grant No. MMY3003 from Janssen-Cilag-Ortho Biotech. The German-speaking Myeloma Multicenter Group was supported by grants from Novartis, Amgen (No. P2004-0060), Chugai, and Roche.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"8 11\",\"pages\":\"\"},\"PeriodicalIF\":14.6000,\"publicationDate\":\"2024-11-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70052\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70052\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70052","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
10 在 827 名患者中,508 人(61%)死亡,78 人(9%)失去随访机会。包括失去随访的患者在内,319 名仍存活的患者的中位随访时间为 11.4 年(四分位数间距:10.2-12.3)。VAD治疗组的12年OS为32%(95% CI:27%-37%),而PAD治疗组为36%(95% CI:31%-41%)(图1A和佐证资料附录第6页)。无论是 Cox 回归分析(HR = 0.87,95% CI:0.73-1.04,p = 0.12,根据 ISS 调整)还是分层对数秩检验(p = 0.15),OS 的差异均无统计学意义。单变量分析以森林图的形式显示在图 1B 中。与之前的报告9、10 一样,ISS 3 期(HR = 0.66,95% CI:0.45-0.97)、del(13q14)(HR = 0.68,95% CI:0.51-0.90)和肾功能损伤(HR = 0.31,95% CI:0.16-0.57)患者亚组显示,PAD 与 VAD 治疗相比,患者有望获益。为了进一步评估选定基线特征对 OS 的预后价值,我们进行了多变量 Cox 回归分析(表 1)。肾功能受损、细胞遗传学不良(仅 GMMG 患者10)患者的 OS,以及根据之前分析的反应状态得出的 OS,见佐证资料 S1:图 1-3,与之前试验的长期随访相比保持不变10。然而,研究组之间的程序有所不同,尤其是在前期异基因移植、串联 ASCT 的使用以及维持治疗的持续时间方面。对自最后一次 ASCT 日期起的 OS 进行的事后分析显示,41%(95% CI:36%-45%)的单次 ASCT 患者和 41%(95% CI:34%-47%)的串联 ASCT 患者的 10 年 OS(HR = 0.99,95% CI:0.81-1.21,P = 0.93)。多中心III期试验HOVON-65/GMMG-HD4的最终长期随访中位数为11.4年,超过35%的患者存活,总体意向治疗人群的10年OS为40%(95% CI:36%-43%)。在单变量分析中,各研究臂的OS差异不大,但在多变量分析中,PAD研究臂的OS优势明显。在肾功能受损的患者中,与 VAD 相比,PAD 的 OS 显著改善,与无肾功能受损的患者相比,OS 相似。同样,PAD 治疗组也克服了 del(17p13) 对预后的负面影响,10 年的 OS 显著提高了 37%,而无 del(17p13) 患者的 OS 为 43%。尽管将化疗加沙利度胺的策略与硼替佐米的策略进行了比较,但在 OS 方面的差异相当小。在复发性 MM 中使用新型疗法可能会部分克服一线疗法疗效较差的问题。与 PAD 组相比,VAD 组首次复发患者使用硼替佐米的比例确实更高(60% 对 33%)10。由于早期复发的患者通常具有高危特征,而在复发时这些新型、更有效的药物可能尚未上市,这可能在一定程度上解释了我们的 OS 结果,尤其是在高危 MM 患者中,并支持对具有高危特征的患者采用更强烈的诱导治疗的风险适应策略。然而,在有 del(17p13) 或肾功能损害的亚组患者中,观察到了 OS 的改善。此外,相当一部分患者存活了 12 年甚至更长时间,这表明目前的 MM 治疗策略是有效的,并强调了在未来试验中进行长期随访分析的重要性。
Bortezomib before and after high-dose therapy in transplant-eligible patients with newly diagnosed multiple myeloma: Long-term overall survival after more than 10 years of follow-up from the phase III HOVON-65/GMMG-HD4 trial
Life expectancy in patients with multiple myeloma (MM) has increased due to the availability of effective drugs such as proteasome inhibitors (PIs),1, 2 immunomodulatory drugs (IMiDs),3-5 and more recently, monoclonal antibodies.6-8
While the progression-free survival (PFS) rates and the depth of response increase with the use of modern multi-drug combinations, it is not clear whether these effects will translate into an improved long-term overall survival (OS). To draw such conclusions, long-term follow-up analyses from trials are needed as comparators for future trials. Here, we report on the long-term overall survival of the HOVON-65/GMMG-HD4 trial including the OS after more than 10 years, and the role of established prognostic factors.
The investigator-sponsored, open-label, randomized HOVON-65/GMMG-HD4 phase III trial was conducted by the Dutch-Belgian Cooperative Trial Group for Hematology Oncology (HOVON) and the German-speaking Myeloma Multicenter Group (GMMG) in 75 centers in the Netherlands, Belgium, and Germany from May 2005 to May 2008 and included 827 eligible patients. The trial was registered at www.trialregister.nl (until June 2022) and https://trialsearch.who.int/ as NTR213, at www.isrctn.com as ISRCTN64455289 and at www.clinicaltrialsregister.eu as EudraCT2004-000944-26. The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).
Initial results of the trial have been published and include a detailed study protocol, inclusion and exclusion criteria, randomization procedures and toxicities,9 and results after a median follow-up of 96 months.10 After that, only OS data were collected on which we here report the final long-term survival data.
The aim of the trial was to investigate the use of bortezomib (BTZ) in induction and maintenance compared to treatment with classical cytotoxic agents as induction and thalidomide maintenance in transplant-eligible patients regarding the primary endpoint PFS, while OS was a secondary endpoint. Patients were randomized 1:1 to receive either vincristine, adriamycin, and dexamethasone (VAD) as induction therapy, followed by high-dose chemotherapy with melphalan and autologous stem-cell transplantation (ASCT), followed by maintenance therapy with thalidomide (VAD arm). In the PAD arm, BTZ, adriamycin, and dexamethasone were used in induction, followed by ASCT and maintenance with BTZ. Patients were stratified by center and International Staging System (ISS, I vs. II vs. III). A single ASCT was planned in the HOVON group, whereas in the GMMG, a tandem ASCT was planned. Patients with an HLA-identical sibling could proceed to allogeneic stem cell transplantation (alloSCT) after the first ASCT.
For the current exploratory analysis, the data available at the final database lock were used (as of July 4, 2019). OS was calculated from randomization until death from any cause, censoring patients alive at the date of last contact.9 OS was estimated by the Kaplan–Meier method, and 95% confidence intervals (CIs) were constructed. The formal test for difference in OS between the two treatment arms was done with a Cox regression analysis with adjustment for the stratification factor ISS. HRs and corresponding 95% CIs were determined. Kaplan–Meier curves were generated to illustrate survival. All analyses were performed on the intention-to-treat population. All reported p-values are two-sided and have not been adjusted for multiple testing. A detailed summary of the trial, eligibility criteria, treatment, response assessment, endpoints, and statistical analysis can be found in the Supporting Information Appendix (pages 3–5) and has been published previously.9, 10
From May 2005 to May 2008, 833 patients were randomly assigned 1:1 to the treatment arms, with 413 and 414 eligible patients being randomized to the VAD and PAD arm, respectively. Six patients were ineligible and excluded from all analyses. Baseline characteristics were reported previously and were evenly distributed.9
Since July 2011, all patients are in follow-up. Differences in the applied treatments between the HOVON and GMMG study groups have been described before.9, 10 In short, in the HOVON group, the number of patients receiving an allogeneic stem cell transplantation was higher (HOVON 60 patients vs. GMMG 2 patients), while in the GMMG study group, more patients received an upfront tandem ASCT (GMMG 273 patients; HOVON 2 patients). Maintenance therapy according to the protocol was initiated in 217 patients in the HOVON group and in 283 patients in the GMMG group with a longer duration of study in the GMMG group.10 A consort diagram for each study group (HOVON and GMMG) and data on documented systemic treatment after the first relapse/progression for MM have been reported previously.10
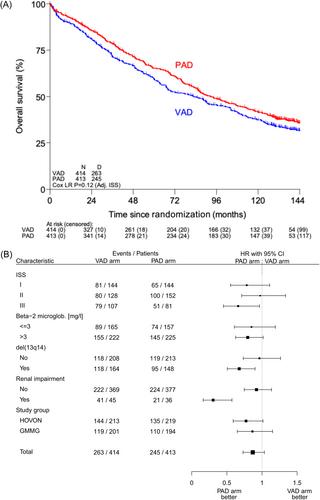
Of the 827 patients, 508 (61%) have died and 78 (9%) patients were lost to follow-up. The median follow-up of the 319 patients still alive including the patients lost to follow-up is 11.4 years (inter-quartile range: 10.2–12.3). The 12-year OS in the VAD arm was 32% (95% CI: 27%–37%) versus 36% (95% CI: 31%–41%) in the PAD arm (Figure 1A and Supporting Information Appendix page 6). The difference in OS was not statistically significant, neither in the Cox regression analysis (HR = 0.87, 95% CI: 0.73–1.04, p = 0.12, adjusted for ISS) nor with the stratified log-rank test (p = 0.15). Univariable analyses are shown as forest plots in Figure 1B. As in the previous reports,9, 10 patient subgroups with ISS stage 3 (HR = 0.66, 95% CI: 0.45–0.97), del(13q14) (HR = 0.68, 95% CI: 0.51–0.90), and renal impairment (HR = 0.31, 95% CI: 0.16–0.57) showed a promising benefit from PAD versus VAD treatment. To further assess the prognostic value of selected baseline characteristics on OS, multivariable Cox regression analysis was performed (Table 1). This analysis revealed a statistically significant OS benefit in favor of the PAD versus VAD arm (HR = 0.84, 95% CI: 0.70–1.00, p = 0.048).
OS on patients with renal impairment, adverse cytogenetics (GMMG patients only10), and according to response status as previously analyzed are shown in Supporting Information S1: Figures 1–3 and remained unchanged with regard to the previous long-term follow-up of the trial.10 In this trial, the use of single versus tandem ASCT was not determined as per the study protocol. However, the procedures between the study groups differed especially regarding upfront allogeneic transplantation, the use of tandem ASCT, and the duration of maintenance therapy.10 A post hoc analysis of OS from the date of the last ASCT showed a 10-year OS for 41% (95% CI: 36%–45%) of patients after single, and 41% (95% CI: 34%–47%) of patients after tandem ASCT (HR = 0.99, 95% CI: 0.81–1.21, p = 0.93).
In this final long-term follow-up of the multicenter, phase III trial HOVON-65/GMMG-HD4 with a median follow-up of 11.4 years, more than 35% of patients are alive, and 10-year OS of the overall intention-to-treat population is 40% (95% CI: 36%–43%). OS did not differ significantly between the study arms in univariable analyses but showed a significant OS advantage for the PAD arm in a multivariable analysis. Treatment in the PAD arm led to improved PFS as was already shown in the previous analyses.9, 10 In patients with renal impairment, OS improved significantly with PAD compared to VAD, resulting in a similar OS as compared to patients without renal impairment. Similarly, the negative prognostic impact of del(17p13) was overcome in the PAD arm with a remarkable 37% OS at 10 years compared to 43% in patients without del(17p13).
Whether the use of a tandem ASCT improves the outcome was extensively elaborated and discussed in an earlier analysis of this study.10 Because of the described confounders it is not possible to draw a definite conclusion about the efficacy of a tandem ASCT compared to a single ASCT from this trial.
Despite comparing chemotherapy plus thalidomide-based to a bortezomib-based strategy, the difference regarding OS is rather small. Likely, a less effective therapy during the first line might be partially overcome by the use of novel therapies in relapsed MM. Bortezomib was indeed used in a higher number of patients at first relapse in the VAD as compared to the PAD arm (60% vs. 33%).10 Several novel agents have been developed for MM treatment after the completion of this trial.2, 6, 7 Therefore, patients with a longer PFS after first-line treatment may have been more likely to be treated with these novel agents after relapse than patients with an early relapse. Since patients with early relapse are usually patients with high-risk features, and the fact that at the time of relapse these novel, more effective agents may not have been available yet, this may in part explain our OS results, particularly in high-risk MM, and support risk-adapted strategies with more intense induction therapies for patients with high-risk features.11 Yet, long-term OS as an outcome measure remains important to elucidate differences in therapeutic strategies.
In summary, in this final long-term follow-up analysis, the primary analysis did not show a statistically significant improvement in OS. However, improvement of OS in subgroups of patients with a del(17p13) or renal impairment was observed. Furthermore, the survival of a substantial fraction of patients for 12 years and longer indicates the effectiveness of current treatment strategies for MM and underlines the importance of long-term follow-up analysis in future trials.
Pieter Sonneveld, Peter Brossart, Sonja Zweegman, Gerard M. J. Bos, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in conception and design. Bronno van der Holt, Uta Bertsch, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in administrative support. Pieter Sonneveld, Hans J. Salwender, Sonja Zweegman, Katja C. Weisel, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Jens Hillengass, Marc S. Raab, Christine Hanoun, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in provision of study materials or patients. Pieter Sonneveld, Peter Brossart, Uta Bertsch, Hans J. Salwender, Sonja Zweegman, Annemiek Broijl, Axel Nogai, Katja C. Weisel, Jens Hillengass, Marc S. Raab, Elias K. Mai, Sandra Croockewit, Gerard M. J. Bos, Marian Stevens-Kroef, Christoph Scheid, Anna Jauch, Thomas Hielscher, Christine Hanoun, Paula Ypma, Henk M. Lokhorst, and Hartmut Goldschmidt were involved in collection and assembly of data. Elias K. Mai, Axel Nogai, Bronno van der Holt, Sonja Zweegman, Marian Stevens-Kroef, Christoph Scheid, Paula Ypma, Thomas Hielscher, Hartmut Goldschmidt, and Pieter Sonneveld were involved in data analysis and interpretation. Elias K. Mai, Axel Nogai, and Bronno van der Holt were involved in writing of the first manuscript draft. All authors involved in manuscript editing and writing, final approval of manuscript.
Elias K. Mai reports consulting or advisory role with Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; honoraria from Amgen, BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Pfizer, Sanofi, Stemline, and Takeda; research funding from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, and Takeda; and travel accommodations and expenses from BMS/Celgene, GlaxoSmithKline, Janssen-Cilag, Sanofi, Stemline, and Takeda. Axel Nogai reports consulting or advisory role with Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi and GSK; honoraria from Celgene, Roche, Takeda, Alexion, Janssen, BMS, Sanofi, and GSK; research support from BMS, Janssen, and Celgene; and travel accommodations and expenses from Takeda, Janssen, Alexion, and Amgen. Bronno van der Holt reports honoraria for data safety monitoring board membership from IFM. Sonja Zweegman reports consulting or advisory role with Janssen, BMS, Sanofi, Oncopeptides, and GSK; and research funding from Takeda and Janssen. Katja C. Weisel reports consulting or advisory role with Abbvie, Amgen, Adaptive Biotech, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Oncopeptides, Pfizer, Regeneron, Roche Pharma, Sanofi, Takeda, and Menarini; honoraria from Abbvie, Amgen, Adaptive Biotech, Astra Zeneca, Bristol Myers Squibb/Celgene, BeiGene, Janssen, GlaxoSmithKline, Karyopharm, Novartis, Oncopeptides, Pfizer, Roche Pharma, Sanofi, Stemline, Takeda, and Menarini; and research funding from Abbvie, Amgen, Bristol Myers Squibb/Celgene, Janssen, GlaxoSmithKline, Pfizer, Sanofi, and Takeda. Jens Hillengass reports advisory role with Prothena, Sebia, and Regeneron; honoraria from Targeted Oncology; and member of data safety monitoring boards with Janssen. Marc S. Raab reports consulting or advisory role with BMS, Amgen, GSK, Janssen, Sanofi, Pfizer, AbbVie, and Takeda; research funding from BMS, Janssen, Sanofi, and Heidelberg Pharma; travel accommodation and expenses from BMS, Amgen, and Janssen; and honoraria from BMS, Janssen, AbbVie, and Sanofi. Annemiek Broijl reports honoraria from Amgen, Sanofi, Janssen, and BMS. Peter Brossart reports consulting or advisory role from Astra-Zeneca, BMS, MSD, BeiGene, and Gilead; research funding from BMS; and honoraria from Gilead, MSD, BMS, and Astra-Zeneca. Christoph Scheid reports consulting or advisory role from Bristol Myers Squibb, GlaxoSmithKline, Janssen, Pfizer, Roche, and Takeda; honoraria from Amgen, Bristol Myers Squibb, GlaxoSmithKline, Janssen, MSD, Novartis, Roche, Sanofi, and Takeda; research funding from Janssen, and Takeda; and travel accommodation and expenses from Bristol Myers Squibb, Janssen, Sanofi Aventis, and Takeda. Hans J. Salwender reports consulting or advisory role with Amgen, AstraZeneca, Bristol Myers Squibb/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Sanofi, and Stemline; honoraria from Abbvie, Amgen, AstraZeneca, Bristol Myers SquibbMS/Celgene, Genzyme, GSK, Janssen Cilag, Oncopeptides, Pfizer, Roche, Sanofi, Stemline, and Takeda; and travel accommodation and expenses from Amgen, Bristol Myers Squibb/Celgene, Janssen Cilag, and Sanofi. Hartmut Goldschmidt reports consulting or advisory role with Amgen, BMS, Janssen, Sanofi, and Adaptive Biotechnology; honoraria from Amgen, BMS, Chugai, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; research funding from Amgen, BMS, Celgene, GlycoMimetics Inc., GlaxoSmithKline, Heidelberg Pharma, Hoffmann-La Roche, Karyopharm, Janssen, Incyte Corporation, Millenium Pharmaceuticals Inc., Molecular Partners, Merck Sharp and Dohme, MorphoSys AG, Pfizer, Sanofi, Takeda, and Novartis; travel accommodations and expenses from Amgen, BMS, GlaxoSmithKline, Janssen, Novartis, Sanofi, and Pfizer; grants from Amgen, Array Biopharma/Pfizer, BMS/Celgene, Chugai, Dietmar-Hopp-Foundation, Janssen, Johns Hopkins University, Mundipharma GmbH, and Sanofi. Pieter Sonneveld reports advisory role with Amgen, BMS, Celgene, Janssen, Karyopharm, and Pfizer; research funding from Amgen, BMS, Janssen, and Karyopharm. All other authors declare no competing interests.
The ethics committees of the Erasmus University Medical Center, the University of Heidelberg, and all participating sites approved this trial. All patients gave written informed consent. The study was conducted in accordance with the European Clinical Trial Directive (2005) and the Declaration of Helsinki (1996).
The HOVON-65/GMMG-HD4 trial was supported by the Dutch Cancer Foundation, the German Federal Ministry of Education and Research, and unrestricted Grant No. MMY3003 from Janssen-Cilag-Ortho Biotech. The German-speaking Myeloma Multicenter Group was supported by grants from Novartis, Amgen (No. P2004-0060), Chugai, and Roche.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
