{"title":"对免疫调节治疗有反应的晚发性肌病:没有神经节桿菌的散发性晚发性神经节桿菌肌病?","authors":"Menachem Sadeh, Yakov Fellig, Ron Dabby","doi":"10.1136/bmjno-2024-000892","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Late-onset sporadic nemaline myopathy (SLONM) is a rare, treatable or potentially life-threatening muscle disorder that typically manifests late in life and is characterised by the presence of nemaline rods within muscle fibres, serving as the hallmark of the disease and the key to diagnosis.</p><p><strong>Methods: </strong>We report a case of an elderly patient with subacute onset of severe weakness affecting the upper and lower limbs, neck extensors and abdominal muscles. A comprehensive laboratory workup was performed.</p><p><strong>Results: </strong>Muscle biopsies showed nonspecific myopathic changes without inflammation, and electron microscopy did not reveal rods or aggregates. The laboratory workup was unremarkable except for the detection of monoclonal gammopathy of undetermined significance. Steroid treatment was ineffective; however, there was a notable positive response to intravenous immunoglobulins. The neurological findings, subacute course, normal creatine kinase levels, presence of monoclonal gammopathy of unknown significance and responsiveness to immunoglobulin treatment but not to steroids align with the characteristics of SLONM.</p><p><strong>Conclusion: </strong>We propose that the diagnosis of SLONM should be considered even in the absence of nemaline rods in muscle biopsy, and this should not impede the consideration of immunomodulatory treatment. Future progress in understanding the pathogenetic basis of SLONM may reduce reliance on pathological findings in muscle biopsies for establishing the diagnosis.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"6 2","pages":"e000892"},"PeriodicalIF":2.6000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11575228/pdf/","citationCount":"0","resultStr":"{\"title\":\"Late-onset myopathy responsive to immunomodulatory treatment: sporadic late-onset nemaline myopathy without nemaline rods?\",\"authors\":\"Menachem Sadeh, Yakov Fellig, Ron Dabby\",\"doi\":\"10.1136/bmjno-2024-000892\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Late-onset sporadic nemaline myopathy (SLONM) is a rare, treatable or potentially life-threatening muscle disorder that typically manifests late in life and is characterised by the presence of nemaline rods within muscle fibres, serving as the hallmark of the disease and the key to diagnosis.</p><p><strong>Methods: </strong>We report a case of an elderly patient with subacute onset of severe weakness affecting the upper and lower limbs, neck extensors and abdominal muscles. A comprehensive laboratory workup was performed.</p><p><strong>Results: </strong>Muscle biopsies showed nonspecific myopathic changes without inflammation, and electron microscopy did not reveal rods or aggregates. The laboratory workup was unremarkable except for the detection of monoclonal gammopathy of undetermined significance. Steroid treatment was ineffective; however, there was a notable positive response to intravenous immunoglobulins. The neurological findings, subacute course, normal creatine kinase levels, presence of monoclonal gammopathy of unknown significance and responsiveness to immunoglobulin treatment but not to steroids align with the characteristics of SLONM.</p><p><strong>Conclusion: </strong>We propose that the diagnosis of SLONM should be considered even in the absence of nemaline rods in muscle biopsy, and this should not impede the consideration of immunomodulatory treatment. Future progress in understanding the pathogenetic basis of SLONM may reduce reliance on pathological findings in muscle biopsies for establishing the diagnosis.</p>\",\"PeriodicalId\":52754,\"journal\":{\"name\":\"BMJ Neurology Open\",\"volume\":\"6 2\",\"pages\":\"e000892\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2024-11-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11575228/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Neurology Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjno-2024-000892\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2024-000892","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Late-onset myopathy responsive to immunomodulatory treatment: sporadic late-onset nemaline myopathy without nemaline rods?
Background: Late-onset sporadic nemaline myopathy (SLONM) is a rare, treatable or potentially life-threatening muscle disorder that typically manifests late in life and is characterised by the presence of nemaline rods within muscle fibres, serving as the hallmark of the disease and the key to diagnosis.
Methods: We report a case of an elderly patient with subacute onset of severe weakness affecting the upper and lower limbs, neck extensors and abdominal muscles. A comprehensive laboratory workup was performed.
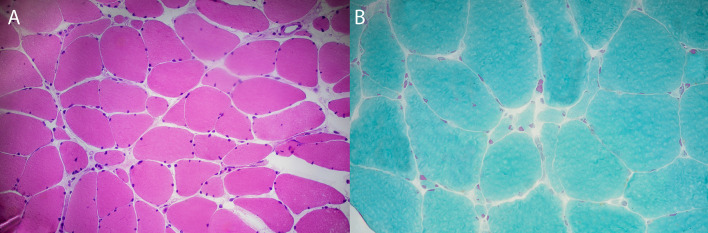
Results: Muscle biopsies showed nonspecific myopathic changes without inflammation, and electron microscopy did not reveal rods or aggregates. The laboratory workup was unremarkable except for the detection of monoclonal gammopathy of undetermined significance. Steroid treatment was ineffective; however, there was a notable positive response to intravenous immunoglobulins. The neurological findings, subacute course, normal creatine kinase levels, presence of monoclonal gammopathy of unknown significance and responsiveness to immunoglobulin treatment but not to steroids align with the characteristics of SLONM.
Conclusion: We propose that the diagnosis of SLONM should be considered even in the absence of nemaline rods in muscle biopsy, and this should not impede the consideration of immunomodulatory treatment. Future progress in understanding the pathogenetic basis of SLONM may reduce reliance on pathological findings in muscle biopsies for establishing the diagnosis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
