Hong-Da Zhang, Lei Ding, Li-Jie Mi, Ai-Kai Zhang, Yuan-Dong Liu, Xiang-Nan Li, Xin-Xin Yan, Yu-Jing Shen, Min Tang
{"title":"新发心房颤动对重症患者死亡率的影响","authors":"Hong-Da Zhang, Lei Ding, Li-Jie Mi, Ai-Kai Zhang, Yuan-Dong Liu, Xiang-Nan Li, Xin-Xin Yan, Yu-Jing Shen, Min Tang","doi":"10.2147/CLEP.S485411","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia in critically ill patients and significantly impacts mortality. This study sought to evaluate the impact of new-onset AF on mortality in a critically ill population.</p><p><strong>Methods: </strong>This study identified 48018 adult patients admitted to the ICU from the Medical Information Mart for Intensive Care (MIMIC)-IV database. Patients were categorized as no AF, pre-existing AF, or new-onset AF. We analyzed mortality at 3 months, 6 months, and 1 year.</p><p><strong>Results: </strong>Overall, 31,562 (65.73%) patients had no AF, 4877 (10.16%) had pre-existing AF, and 11,579 (24.11%) had new-onset AF. Median ages were 61.47 years (no AF), 76.12 years (pre-existing AF), and 75.26 years (new-onset AF). New-onset AF was associated with the highest mortality rates: 25.16% at 3 months, 29.23% at 6 months, and 34.04% at 1 year, compared to 17.94%, 22.55%, and 28.52% for pre-existing AF, and 14.54%, 17.25%, and 20.69% for no AF respectively (p < 0.001 for all). Multivariate Cox regression indicated that new-onset AF significantly increased the risk of 1-year mortality by 15.5% compared to no AF (HR: 1.155, 95% CI: 1.101-1.212; p < 0.001) and by 23.9% compared to pre-existing AF (HR: 1.239, 95% CI: 1.164-1.318; p < 0.001). Kaplan-Meier analysis confirmed lower survival probabilities for new-onset AF over one year compared to the other groups (p < 0.001).</p><p><strong>Conclusion: </strong>In patients with critical illness, new-onset AF is associated with an increased risk of mortality compared with pre-existing AF or no AF.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"16 ","pages":"811-822"},"PeriodicalIF":4.3000,"publicationDate":"2024-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587791/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of New-Onset Atrial Fibrillation on Mortality in Critically Ill Patients.\",\"authors\":\"Hong-Da Zhang, Lei Ding, Li-Jie Mi, Ai-Kai Zhang, Yuan-Dong Liu, Xiang-Nan Li, Xin-Xin Yan, Yu-Jing Shen, Min Tang\",\"doi\":\"10.2147/CLEP.S485411\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia in critically ill patients and significantly impacts mortality. This study sought to evaluate the impact of new-onset AF on mortality in a critically ill population.</p><p><strong>Methods: </strong>This study identified 48018 adult patients admitted to the ICU from the Medical Information Mart for Intensive Care (MIMIC)-IV database. Patients were categorized as no AF, pre-existing AF, or new-onset AF. We analyzed mortality at 3 months, 6 months, and 1 year.</p><p><strong>Results: </strong>Overall, 31,562 (65.73%) patients had no AF, 4877 (10.16%) had pre-existing AF, and 11,579 (24.11%) had new-onset AF. Median ages were 61.47 years (no AF), 76.12 years (pre-existing AF), and 75.26 years (new-onset AF). New-onset AF was associated with the highest mortality rates: 25.16% at 3 months, 29.23% at 6 months, and 34.04% at 1 year, compared to 17.94%, 22.55%, and 28.52% for pre-existing AF, and 14.54%, 17.25%, and 20.69% for no AF respectively (p < 0.001 for all). Multivariate Cox regression indicated that new-onset AF significantly increased the risk of 1-year mortality by 15.5% compared to no AF (HR: 1.155, 95% CI: 1.101-1.212; p < 0.001) and by 23.9% compared to pre-existing AF (HR: 1.239, 95% CI: 1.164-1.318; p < 0.001). Kaplan-Meier analysis confirmed lower survival probabilities for new-onset AF over one year compared to the other groups (p < 0.001).</p><p><strong>Conclusion: </strong>In patients with critical illness, new-onset AF is associated with an increased risk of mortality compared with pre-existing AF or no AF.</p>\",\"PeriodicalId\":10362,\"journal\":{\"name\":\"Clinical Epidemiology\",\"volume\":\"16 \",\"pages\":\"811-822\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-11-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11587791/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CLEP.S485411\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S485411","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Impact of New-Onset Atrial Fibrillation on Mortality in Critically Ill Patients.
Background: Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia in critically ill patients and significantly impacts mortality. This study sought to evaluate the impact of new-onset AF on mortality in a critically ill population.
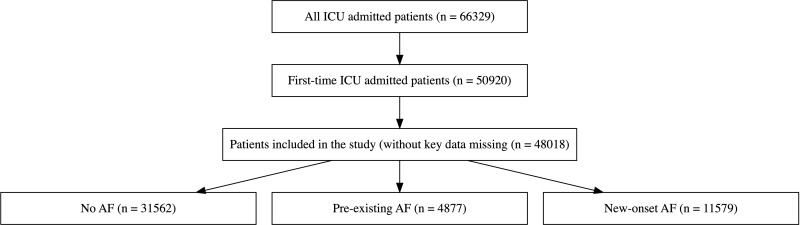
Methods: This study identified 48018 adult patients admitted to the ICU from the Medical Information Mart for Intensive Care (MIMIC)-IV database. Patients were categorized as no AF, pre-existing AF, or new-onset AF. We analyzed mortality at 3 months, 6 months, and 1 year.
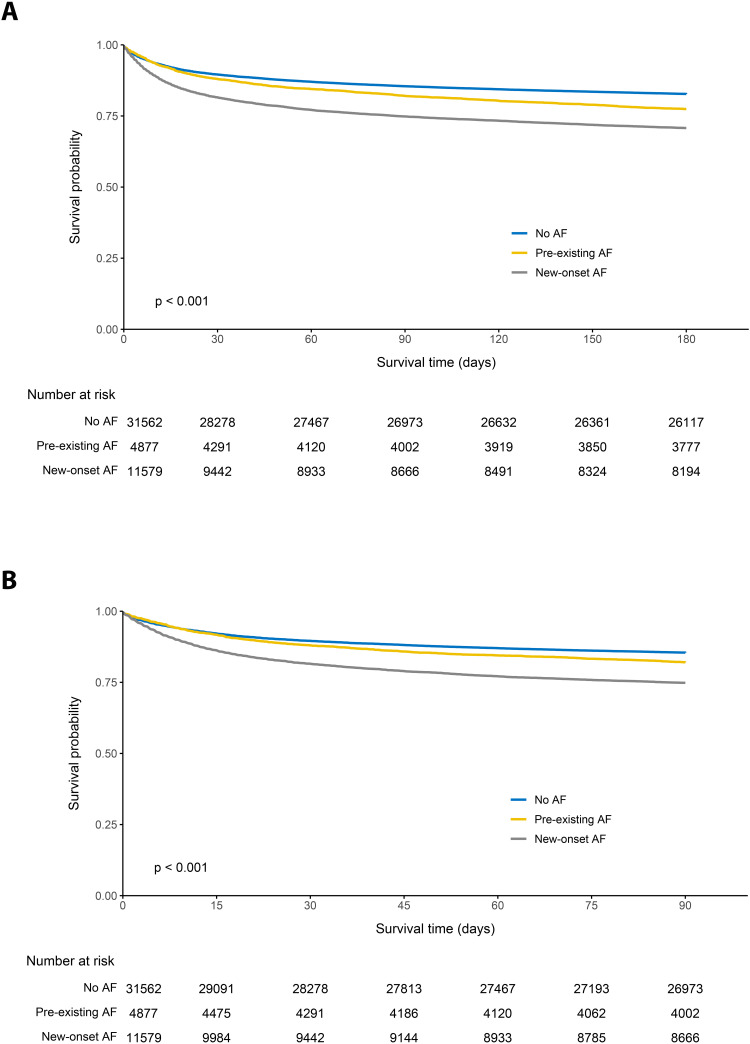
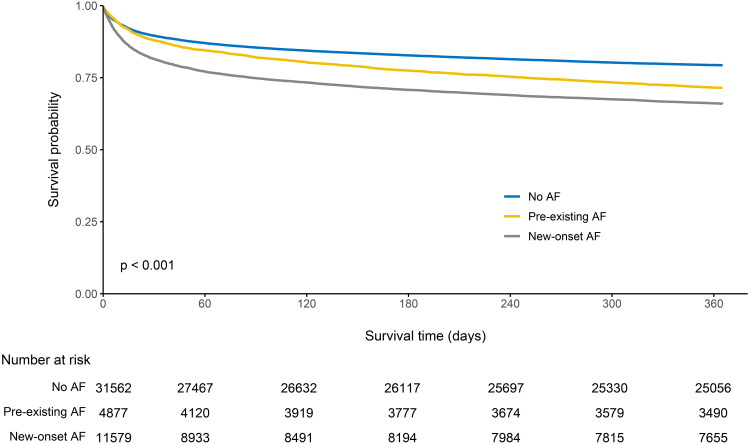
Results: Overall, 31,562 (65.73%) patients had no AF, 4877 (10.16%) had pre-existing AF, and 11,579 (24.11%) had new-onset AF. Median ages were 61.47 years (no AF), 76.12 years (pre-existing AF), and 75.26 years (new-onset AF). New-onset AF was associated with the highest mortality rates: 25.16% at 3 months, 29.23% at 6 months, and 34.04% at 1 year, compared to 17.94%, 22.55%, and 28.52% for pre-existing AF, and 14.54%, 17.25%, and 20.69% for no AF respectively (p < 0.001 for all). Multivariate Cox regression indicated that new-onset AF significantly increased the risk of 1-year mortality by 15.5% compared to no AF (HR: 1.155, 95% CI: 1.101-1.212; p < 0.001) and by 23.9% compared to pre-existing AF (HR: 1.239, 95% CI: 1.164-1.318; p < 0.001). Kaplan-Meier analysis confirmed lower survival probabilities for new-onset AF over one year compared to the other groups (p < 0.001).
Conclusion: In patients with critical illness, new-onset AF is associated with an increased risk of mortality compared with pre-existing AF or no AF.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
