Portia Smallbone, Mallika Sekhar, Samer A. Srour, Jeremy L. Ramdial, Crystal L. Carmicheal Kusy, Elizabeth J. Shpall, Uday R. Popat
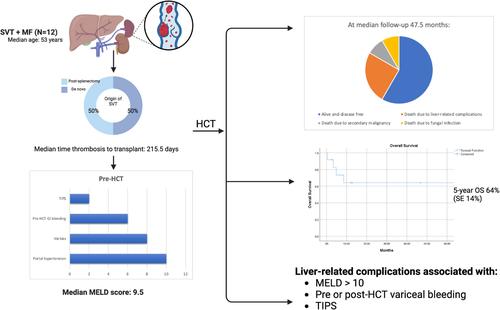
{"title":"骨髓纤维化和内脏静脉血栓患者的造血干细胞移植:一个病例系列","authors":"Portia Smallbone, Mallika Sekhar, Samer A. Srour, Jeremy L. Ramdial, Crystal L. Carmicheal Kusy, Elizabeth J. Shpall, Uday R. Popat","doi":"10.1002/ajh.27542","DOIUrl":null,"url":null,"abstract":"<p>\n \n <figure>\n <div><picture>\n <source></source></picture><p></p>\n </div>\n </figure>\n </p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"100 2","pages":"305-309"},"PeriodicalIF":9.9000,"publicationDate":"2024-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27542","citationCount":"0","resultStr":"{\"title\":\"Hematopoietic Stem Cell Transplantation in Patients With Myelofibrosis and Splanchnic Vein Thrombosis: A Case Series\",\"authors\":\"Portia Smallbone, Mallika Sekhar, Samer A. Srour, Jeremy L. Ramdial, Crystal L. Carmicheal Kusy, Elizabeth J. Shpall, Uday R. Popat\",\"doi\":\"10.1002/ajh.27542\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>\\n \\n <figure>\\n <div><picture>\\n <source></source></picture><p></p>\\n </div>\\n </figure>\\n </p>\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"100 2\",\"pages\":\"305-309\"},\"PeriodicalIF\":9.9000,\"publicationDate\":\"2024-12-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27542\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27542\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27542","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
