Xun Tian , Danhui Weng , Ye Chen , Yi Wang , Xiao Li , Xin Wang , Chen Cao , Danni Gong , Zhen Zeng , Qiongyan Wu , Xueqian Wang , Peng Wu , Lu Fan , Qinghua Zhang , Hui Wang , Zheng Hu , Xiaodong Cheng , Ding Ma
{"title":"宫颈癌初筛对HPV整合状况的风险评估和分诊策略:一项前瞻性队列研究的5年随访。","authors":"Xun Tian , Danhui Weng , Ye Chen , Yi Wang , Xiao Li , Xin Wang , Chen Cao , Danni Gong , Zhen Zeng , Qiongyan Wu , Xueqian Wang , Peng Wu , Lu Fan , Qinghua Zhang , Hui Wang , Zheng Hu , Xiaodong Cheng , Ding Ma","doi":"10.1016/j.jncc.2024.08.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>We investigated the relation between man papillomavirus (HPV) integration status and the immediate risk of cervical intraepithelial neoplasia (CIN), as well as the triage strategy based on HPV integration test.</div></div><div><h3>Methods</h3><div>4086 women aged 20 to 65 years in China were enrolled in 2015 for a prospective, population-based, clinical observational study to evaluate the triage performance of HPV integration. Cervical exfoliated cells were collected for HPV testing and cytologic test. If high-risk HPV was positive, HPV integration test was performed at baseline, 2-year and 5-year follow-up.</div></div><div><h3>Results</h3><div>At baseline, HPV integration was positively correlated with the severity of cervical pathology, ranging from 5.0% (15/301) in normal diagnosis, 6.9% (4/58) in CIN1, 31.0% (9/29) in CIN2, 70% (14/20) in CIN3, and 100% (2/2) in cervical cancer (<em>P</em> < 0.001). Compared with cytology, HPV integration exhibits comparable sensitivity and negative predictive value for the diagnosis of CIN3+, higher specificity (92.8% [90.2%–95.4%] vs. 75.5% [71.2%–79.8%], <em>P</em> < 0.001) and higher positive predictive value (36.4% [22.1%–50.6%] vs. 15.2% [8.5%–21.8%], <em>P</em> < 0.001). HPV integration testing strategy yielded a significantly lower colposcopy referral rate than cytology strategy (10.7% [44/410] vs. 27.3% [112/410], <em>P</em> < 0.001). The HPV integration-negative group exhibited the lowest immediate risk for CIN3+ (1.6%) and accounted for the largest proportion of the total population (89.3%), when compared with the normal cytology group (risk, 1.7%; proportion, 72.7%).</div></div><div><h3>Conclusion</h3><div>As a key molecular basis for the development of cervical cancer, HPV integration might be a promising triage strategy for HPV-positive patients.</div></div>","PeriodicalId":73987,"journal":{"name":"Journal of the National Cancer Center","volume":"4 4","pages":"Pages 311-317"},"PeriodicalIF":9.4000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11674434/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk assessment and triage strategy of cervical cancer primary screening on HPV integration status: 5-year follow-up of a prospective cohort study\",\"authors\":\"Xun Tian , Danhui Weng , Ye Chen , Yi Wang , Xiao Li , Xin Wang , Chen Cao , Danni Gong , Zhen Zeng , Qiongyan Wu , Xueqian Wang , Peng Wu , Lu Fan , Qinghua Zhang , Hui Wang , Zheng Hu , Xiaodong Cheng , Ding Ma\",\"doi\":\"10.1016/j.jncc.2024.08.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><div>We investigated the relation between man papillomavirus (HPV) integration status and the immediate risk of cervical intraepithelial neoplasia (CIN), as well as the triage strategy based on HPV integration test.</div></div><div><h3>Methods</h3><div>4086 women aged 20 to 65 years in China were enrolled in 2015 for a prospective, population-based, clinical observational study to evaluate the triage performance of HPV integration. Cervical exfoliated cells were collected for HPV testing and cytologic test. If high-risk HPV was positive, HPV integration test was performed at baseline, 2-year and 5-year follow-up.</div></div><div><h3>Results</h3><div>At baseline, HPV integration was positively correlated with the severity of cervical pathology, ranging from 5.0% (15/301) in normal diagnosis, 6.9% (4/58) in CIN1, 31.0% (9/29) in CIN2, 70% (14/20) in CIN3, and 100% (2/2) in cervical cancer (<em>P</em> < 0.001). Compared with cytology, HPV integration exhibits comparable sensitivity and negative predictive value for the diagnosis of CIN3+, higher specificity (92.8% [90.2%–95.4%] vs. 75.5% [71.2%–79.8%], <em>P</em> < 0.001) and higher positive predictive value (36.4% [22.1%–50.6%] vs. 15.2% [8.5%–21.8%], <em>P</em> < 0.001). HPV integration testing strategy yielded a significantly lower colposcopy referral rate than cytology strategy (10.7% [44/410] vs. 27.3% [112/410], <em>P</em> < 0.001). The HPV integration-negative group exhibited the lowest immediate risk for CIN3+ (1.6%) and accounted for the largest proportion of the total population (89.3%), when compared with the normal cytology group (risk, 1.7%; proportion, 72.7%).</div></div><div><h3>Conclusion</h3><div>As a key molecular basis for the development of cervical cancer, HPV integration might be a promising triage strategy for HPV-positive patients.</div></div>\",\"PeriodicalId\":73987,\"journal\":{\"name\":\"Journal of the National Cancer Center\",\"volume\":\"4 4\",\"pages\":\"Pages 311-317\"},\"PeriodicalIF\":9.4000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11674434/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the National Cancer Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S266700542400084X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the National Cancer Center","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S266700542400084X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/16 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
研究目的我们研究了人乳头瘤病毒(HPV)整合状态与宫颈上皮内瘤变(CIN)即刻风险之间的关系,以及基于HPV整合检测的分诊策略。方法:2015年,我们在中国招募了4086名20至65岁的女性,开展了一项前瞻性、基于人群的临床观察研究,以评估HPV整合的分诊效果。采集宫颈脱落细胞进行HPV检测和细胞学检测。如果高危HPV阳性,则在基线、2年和5年随访时进行HPV整合测试:基线时,HPV整合与宫颈病变的严重程度呈正相关,正常诊断为5.0%(15/301),CIN1为6.9%(4/58),CIN2为31.0%(9/29),CIN3为70%(14/20),宫颈癌为100%(2/2)(P < 0.001)。与细胞学相比,HPV 整合检测对 CIN3+ 诊断的灵敏度和阴性预测值相当,特异性更高(92.8% [90.2%-95.4%] vs. 75.5% [71.2%-79.8%],P < 0.001),阳性预测值更高(36.4% [22.1%-50.6%] vs. 15.2% [8.5%-21.8%],P < 0.001)。HPV整合检测策略的阴道镜检查转诊率明显低于细胞学策略(10.7% [44/410] vs. 27.3% [112/410],P < 0.001)。与细胞学正常组(风险,1.7%;比例,72.7%)相比,HPV 整合阴性组的 CIN3+ 直接风险最低(1.6%),占总人数的比例最大(89.3%):作为宫颈癌发病的关键分子基础,HPV整合可能是对HPV阳性患者进行分诊的一种有前途的策略。
Risk assessment and triage strategy of cervical cancer primary screening on HPV integration status: 5-year follow-up of a prospective cohort study
Objective
We investigated the relation between man papillomavirus (HPV) integration status and the immediate risk of cervical intraepithelial neoplasia (CIN), as well as the triage strategy based on HPV integration test.
Methods
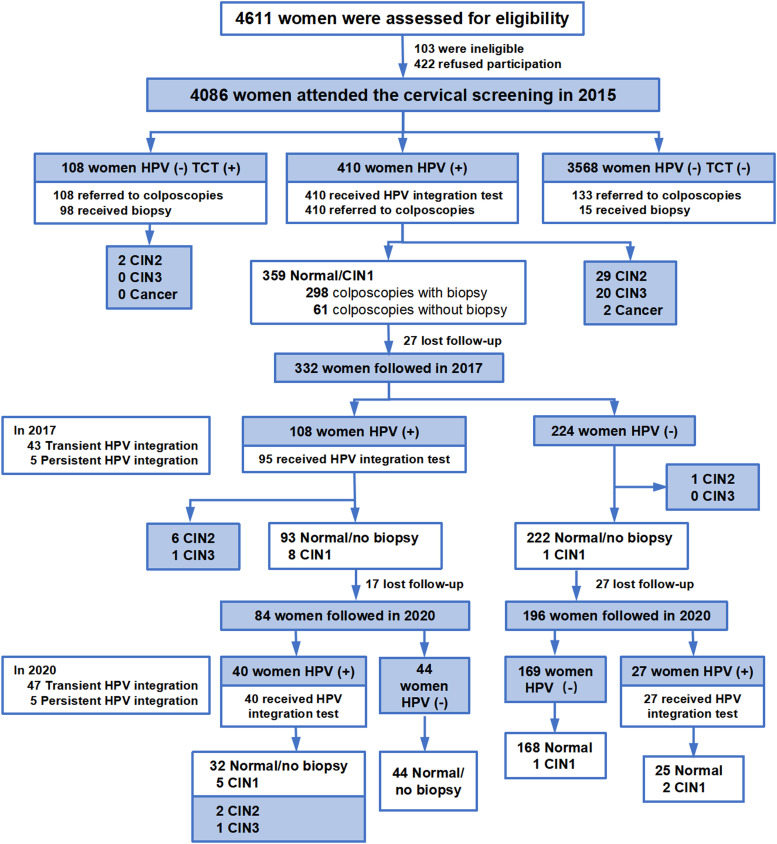
4086 women aged 20 to 65 years in China were enrolled in 2015 for a prospective, population-based, clinical observational study to evaluate the triage performance of HPV integration. Cervical exfoliated cells were collected for HPV testing and cytologic test. If high-risk HPV was positive, HPV integration test was performed at baseline, 2-year and 5-year follow-up.
Results
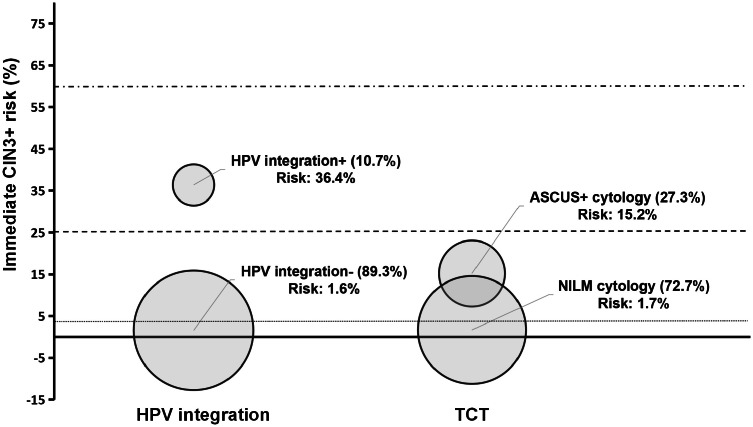
At baseline, HPV integration was positively correlated with the severity of cervical pathology, ranging from 5.0% (15/301) in normal diagnosis, 6.9% (4/58) in CIN1, 31.0% (9/29) in CIN2, 70% (14/20) in CIN3, and 100% (2/2) in cervical cancer (P < 0.001). Compared with cytology, HPV integration exhibits comparable sensitivity and negative predictive value for the diagnosis of CIN3+, higher specificity (92.8% [90.2%–95.4%] vs. 75.5% [71.2%–79.8%], P < 0.001) and higher positive predictive value (36.4% [22.1%–50.6%] vs. 15.2% [8.5%–21.8%], P < 0.001). HPV integration testing strategy yielded a significantly lower colposcopy referral rate than cytology strategy (10.7% [44/410] vs. 27.3% [112/410], P < 0.001). The HPV integration-negative group exhibited the lowest immediate risk for CIN3+ (1.6%) and accounted for the largest proportion of the total population (89.3%), when compared with the normal cytology group (risk, 1.7%; proportion, 72.7%).
Conclusion
As a key molecular basis for the development of cervical cancer, HPV integration might be a promising triage strategy for HPV-positive patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
