Katie Harris , Jessica Gong , Stephen MacMahon , Ying Xu , Sultana Shajahan , Stephen Harrap , Neil Poulter , Michel Marre , Pavel Hamet , Giuseppe Mancia , Craig Anderson , Mark Woodward , John Chalmers
{"title":"根据基线认知功能和其他2型糖尿病患者亚群,随机降压治疗和强化血糖控制对痴呆和认知能力下降的影响:ADVANCE试验的结果","authors":"Katie Harris , Jessica Gong , Stephen MacMahon , Ying Xu , Sultana Shajahan , Stephen Harrap , Neil Poulter , Michel Marre , Pavel Hamet , Giuseppe Mancia , Craig Anderson , Mark Woodward , John Chalmers","doi":"10.1016/j.cccb.2024.100372","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and aims</h3><div>Accumulating evidence indicates that reducing high blood pressure (BP) prevents dementia and mild cognitive impairment (MCI). Furthermore, although diabetes is a risk factor for dementia and MCI, there is uncertainty of the effect of intensive glucose control on these endpoints. This study aimed to determine the effects of BP-lowering (vs placebo) and intensive glucose-lowering (vs standard control) treatments according to baseline cognition and other characteristics on dementia and cognitive decline (CD) in people with type 2 diabetes mellitus (T2DM).</div></div><div><h3>Methods</h3><div>The Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial involved 11,140 individuals with T2DM. The effects of BP-lowering and intensive glucose-lowering treatments were explored in subgroups of baseline Mini-Mental State Examination (MMSE), categorised as cognitively normal (scores ≥28) and cognitive impairment (scores <28). The primary outcome was a composite of dementia/CD that accounted for the competing risk of death. Multinomial regression models, adjusted for common cardiovascular risk factors, were used to estimate odds ratios (OR) with 95 % confidence intervals (CI) of the effects of the treatments on dementia/CD. Homogeneity of effects by subgroups were evaluated using interaction terms in the models. A two-sided p value <0.05 was regarded as statistically significant.</div></div><div><h3>Results</h3><div>BP-lowering treatment (vs. placebo) was associated with a lower odds of dementia/CD in participants with cognitive impairment (OR 0.76, 95 % CI (0.59–0.99)) but not in those cognitively normal (OR 1.05, 95 % CI (0.92–1.21); p for interaction 0.03). Those with a history of cardio-renal-metabolic syndrome did not experience a benefit of active BP lowering treatment compared with placebo on dementia/CD. There were no further subgroup effects of BP-lowering treatment. The effect of intensive glucose lowering (vs standard control) on the odds of dementia/CD did not vary by baseline cognition subgroup. However, it did vary by level of blood glucose at baseline (<7.9 mmol/L OR 1.12, 95 % CI (0.96–1.30) vs ≥ 7.9 mmol/L 0.87 (0.75–1.00); p for interaction 0.02) and duration of T2DM (<10 years OR 0.92 (0.81–1.05) vs ≥10 years 1.16 (0.97–1.38); p for interaction 0.04).</div></div><div><h3>Conclusions</h3><div>This study suggests greater effects of BP-lowering treatment in those with early loss of cognitive function than in those cognitively normal. There were also differential effects of intensive glucose-lowering on dementia and CD according to levels of blood glucose and duration of diabetes in people with T2DM.</div></div><div><h3>Clinical trial registration</h3><div>ADVANCE is registered with ClinicalTrials.gov: number NCT00145925</div></div>","PeriodicalId":72549,"journal":{"name":"Cerebral circulation - cognition and behavior","volume":"8 ","pages":"Article 100372"},"PeriodicalIF":2.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699603/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of randomised blood pressure lowering treatment and intensive glucose control on dementia and cognitive decline according to baseline cognitive function and other subpopulations of individuals with type 2 diabetes: Results from the ADVANCE trial\",\"authors\":\"Katie Harris , Jessica Gong , Stephen MacMahon , Ying Xu , Sultana Shajahan , Stephen Harrap , Neil Poulter , Michel Marre , Pavel Hamet , Giuseppe Mancia , Craig Anderson , Mark Woodward , John Chalmers\",\"doi\":\"10.1016/j.cccb.2024.100372\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and aims</h3><div>Accumulating evidence indicates that reducing high blood pressure (BP) prevents dementia and mild cognitive impairment (MCI). Furthermore, although diabetes is a risk factor for dementia and MCI, there is uncertainty of the effect of intensive glucose control on these endpoints. This study aimed to determine the effects of BP-lowering (vs placebo) and intensive glucose-lowering (vs standard control) treatments according to baseline cognition and other characteristics on dementia and cognitive decline (CD) in people with type 2 diabetes mellitus (T2DM).</div></div><div><h3>Methods</h3><div>The Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial involved 11,140 individuals with T2DM. The effects of BP-lowering and intensive glucose-lowering treatments were explored in subgroups of baseline Mini-Mental State Examination (MMSE), categorised as cognitively normal (scores ≥28) and cognitive impairment (scores <28). The primary outcome was a composite of dementia/CD that accounted for the competing risk of death. Multinomial regression models, adjusted for common cardiovascular risk factors, were used to estimate odds ratios (OR) with 95 % confidence intervals (CI) of the effects of the treatments on dementia/CD. Homogeneity of effects by subgroups were evaluated using interaction terms in the models. A two-sided p value <0.05 was regarded as statistically significant.</div></div><div><h3>Results</h3><div>BP-lowering treatment (vs. placebo) was associated with a lower odds of dementia/CD in participants with cognitive impairment (OR 0.76, 95 % CI (0.59–0.99)) but not in those cognitively normal (OR 1.05, 95 % CI (0.92–1.21); p for interaction 0.03). Those with a history of cardio-renal-metabolic syndrome did not experience a benefit of active BP lowering treatment compared with placebo on dementia/CD. There were no further subgroup effects of BP-lowering treatment. The effect of intensive glucose lowering (vs standard control) on the odds of dementia/CD did not vary by baseline cognition subgroup. However, it did vary by level of blood glucose at baseline (<7.9 mmol/L OR 1.12, 95 % CI (0.96–1.30) vs ≥ 7.9 mmol/L 0.87 (0.75–1.00); p for interaction 0.02) and duration of T2DM (<10 years OR 0.92 (0.81–1.05) vs ≥10 years 1.16 (0.97–1.38); p for interaction 0.04).</div></div><div><h3>Conclusions</h3><div>This study suggests greater effects of BP-lowering treatment in those with early loss of cognitive function than in those cognitively normal. There were also differential effects of intensive glucose-lowering on dementia and CD according to levels of blood glucose and duration of diabetes in people with T2DM.</div></div><div><h3>Clinical trial registration</h3><div>ADVANCE is registered with ClinicalTrials.gov: number NCT00145925</div></div>\",\"PeriodicalId\":72549,\"journal\":{\"name\":\"Cerebral circulation - cognition and behavior\",\"volume\":\"8 \",\"pages\":\"Article 100372\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11699603/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebral circulation - cognition and behavior\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666245024001739\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebral circulation - cognition and behavior","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666245024001739","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/5 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:越来越多的证据表明,降低高血压(BP)可以预防痴呆和轻度认知障碍(MCI)。此外,虽然糖尿病是痴呆和轻度认知障碍的危险因素,但强化血糖控制对这些终点的影响尚不确定。本研究旨在根据基线认知和其他特征确定降压(相对于安慰剂)和强化降糖(相对于标准对照)治疗对2型糖尿病(T2DM)患者痴呆和认知能力下降(CD)的影响。方法:在糖尿病和血管疾病中的作用:Preterax和Diamicron改良释放控制评价(ADVANCE)试验纳入11,140例T2DM患者。在基线迷你精神状态检查(MMSE)的亚组中,研究了降压和强化降糖治疗的效果,分为认知正常(评分≥28)和认知障碍(评分结果:降压治疗(与安慰剂相比)与认知障碍参与者的痴呆/CD发生率较低相关(OR 0.76, 95% CI(0.59-0.99)),但与认知正常参与者无关(OR 1.05, 95% CI (0.92-1.21);P为相互作用0.03)。与安慰剂相比,那些有心肾代谢综合征病史的患者在痴呆/CD方面没有得到主动降压治疗的益处。降压治疗没有进一步的亚组效应。强化降糖(与标准对照)对痴呆/CD几率的影响在基线认知亚组中没有变化。然而,它确实因基线血糖水平而异(结论:这项研究表明,与认知功能正常的人相比,早期认知功能丧失的人降压治疗的效果更大。根据2型糖尿病患者的血糖水平和糖尿病病程,强化降糖对痴呆和CD的影响也存在差异。临床试验注册:ADVANCE在ClinicalTrials.gov注册:编号NCT00145925。
Effect of randomised blood pressure lowering treatment and intensive glucose control on dementia and cognitive decline according to baseline cognitive function and other subpopulations of individuals with type 2 diabetes: Results from the ADVANCE trial
Background and aims
Accumulating evidence indicates that reducing high blood pressure (BP) prevents dementia and mild cognitive impairment (MCI). Furthermore, although diabetes is a risk factor for dementia and MCI, there is uncertainty of the effect of intensive glucose control on these endpoints. This study aimed to determine the effects of BP-lowering (vs placebo) and intensive glucose-lowering (vs standard control) treatments according to baseline cognition and other characteristics on dementia and cognitive decline (CD) in people with type 2 diabetes mellitus (T2DM).
Methods
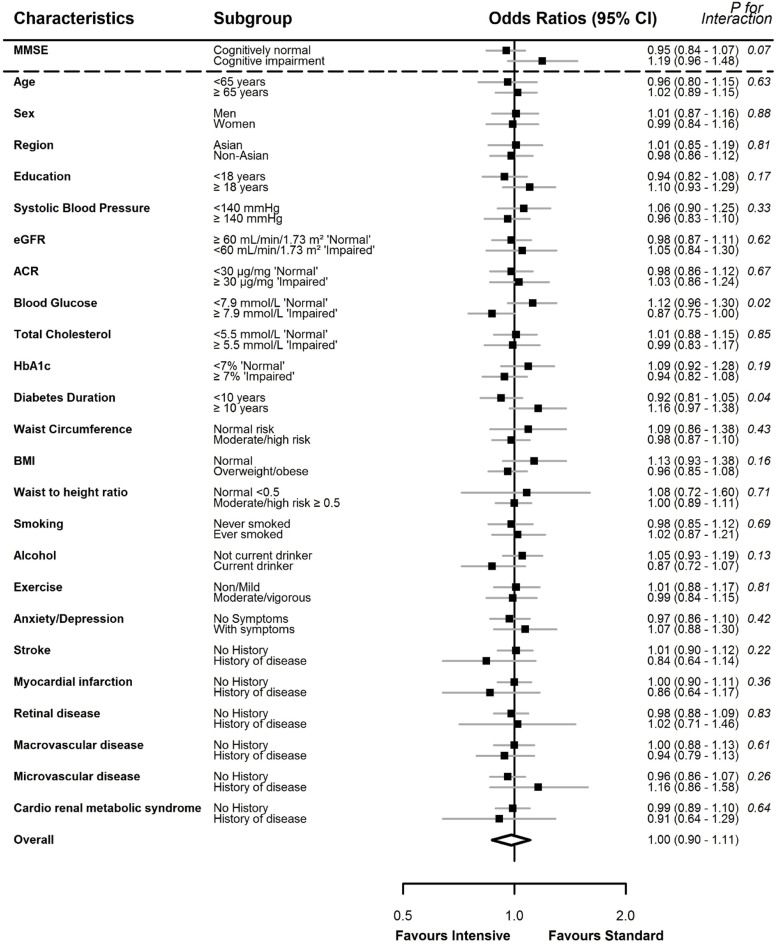
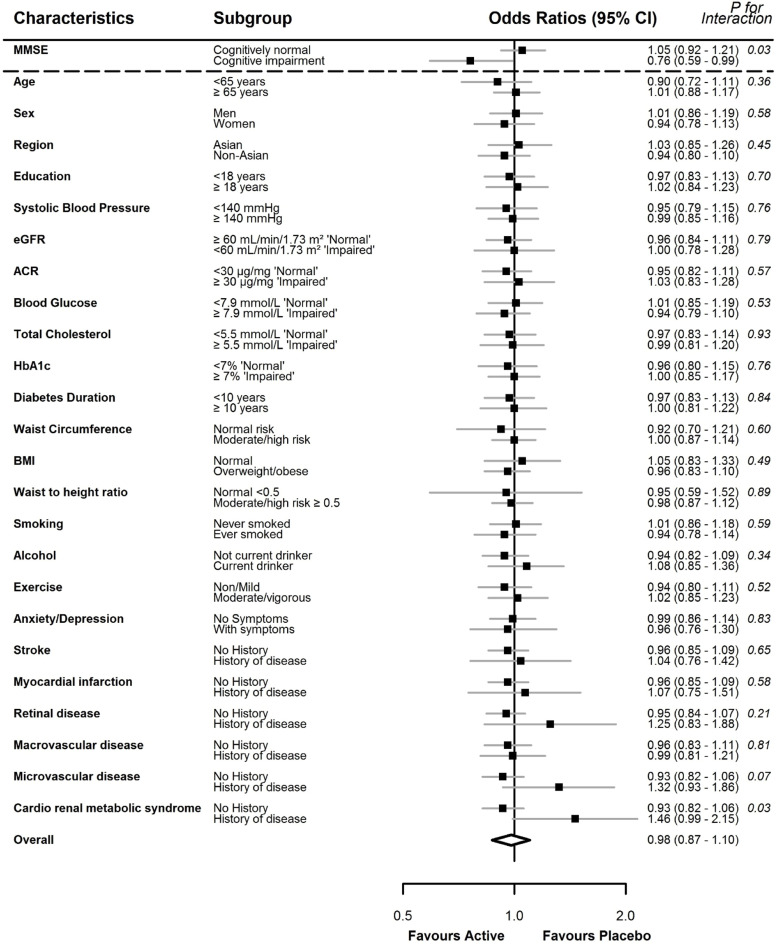
The Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial involved 11,140 individuals with T2DM. The effects of BP-lowering and intensive glucose-lowering treatments were explored in subgroups of baseline Mini-Mental State Examination (MMSE), categorised as cognitively normal (scores ≥28) and cognitive impairment (scores <28). The primary outcome was a composite of dementia/CD that accounted for the competing risk of death. Multinomial regression models, adjusted for common cardiovascular risk factors, were used to estimate odds ratios (OR) with 95 % confidence intervals (CI) of the effects of the treatments on dementia/CD. Homogeneity of effects by subgroups were evaluated using interaction terms in the models. A two-sided p value <0.05 was regarded as statistically significant.
Results
BP-lowering treatment (vs. placebo) was associated with a lower odds of dementia/CD in participants with cognitive impairment (OR 0.76, 95 % CI (0.59–0.99)) but not in those cognitively normal (OR 1.05, 95 % CI (0.92–1.21); p for interaction 0.03). Those with a history of cardio-renal-metabolic syndrome did not experience a benefit of active BP lowering treatment compared with placebo on dementia/CD. There were no further subgroup effects of BP-lowering treatment. The effect of intensive glucose lowering (vs standard control) on the odds of dementia/CD did not vary by baseline cognition subgroup. However, it did vary by level of blood glucose at baseline (<7.9 mmol/L OR 1.12, 95 % CI (0.96–1.30) vs ≥ 7.9 mmol/L 0.87 (0.75–1.00); p for interaction 0.02) and duration of T2DM (<10 years OR 0.92 (0.81–1.05) vs ≥10 years 1.16 (0.97–1.38); p for interaction 0.04).
Conclusions
This study suggests greater effects of BP-lowering treatment in those with early loss of cognitive function than in those cognitively normal. There were also differential effects of intensive glucose-lowering on dementia and CD according to levels of blood glucose and duration of diabetes in people with T2DM.
Clinical trial registration
ADVANCE is registered with ClinicalTrials.gov: number NCT00145925



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
