Piyanuch Kongtim, Piyatida Chumnumsiriwath, Pongthep Vittayawacharin, Deepa Jeyakumar, Benjamin J. Lee, Jean Doh, Shawn P. Griffin, Richard A. Van Etten, Stefan Ciurea
{"title":"布地奈德加入ptc治疗方案预防同种异体干细胞移植后急性胃肠道移植物抗宿主病","authors":"Piyanuch Kongtim, Piyatida Chumnumsiriwath, Pongthep Vittayawacharin, Deepa Jeyakumar, Benjamin J. Lee, Jean Doh, Shawn P. Griffin, Richard A. Van Etten, Stefan Ciurea","doi":"10.1002/ajh.27581","DOIUrl":null,"url":null,"abstract":"Oral budesonide exerts local effects with negligible systemic glucocorticoid activity, due to rapid first-pass metabolism, therefore, could potentially be efficacious in preventing gastrointestinal (GI) acute GVHD (aGVHD). We explored the use of budesonide, added to posttransplant cyclophosphamide (PTCy), tacrolimus, and mycophenolate mofetil, for prevention of GI aGVHD after allogeneic hematopoietic stem cell transplantation (AHSCT) in a prospective observational study and treated 80 patients with a median age of 53 years (range 19–74). Results were compared with a publicly available CIBMTR dataset of 646 patients who received PTCy-based GVHD prophylaxis (CIBMTR Study # GV17-02) (control). Cumulative incidence (CI) of 3-month grade 2–4 and grade 3–4 aGVHD in the budesonide and control groups were 3.8% vs. 34.4% (<i>p</i> < 0.001) and 1.3% vs. 9.8% (<i>p</i> = 0.029), respectively. One-year GRFS (70.5% vs. 31.5%, <i>p</i> < 0.001), PFS (73.4% vs. 52.8%, <i>p</i> = 0.003), and OS (80.1% vs. 64.2%, <i>p</i> = 0.038) were significantly higher in the budesonide group compared with control group. Propensity score-adjusted analyses showed that the addition of budesonide significantly decreased risk of aGVHD grade 2–4 (HR 0.29, <i>p</i> < 0.001), grade 3–4 (HR 0.12, <i>p</i> = 0.045), and cGVHD (HR 0.22, <i>p</i> < 0.001), which resulted in better GRFS (HR 0.38, <i>p</i> < 0.001), PFS (HR 0.58, <i>p</i> = 0.012), and OS (HR 0.72, <i>p</i> = 0.044). Similar results were found when using propensity score-matched analysis restricted to recipients of haploidentical transplantation. In conclusion, addition of budesonide to PTCy-based GVHD prophylaxis is safe and effective in preventing severe acute GI GVHD with significantly improved GRFS. These results could facilitate transition to peripheral blood grafts for all allogeneic transplant recipients.","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"13 1","pages":""},"PeriodicalIF":10.1000,"publicationDate":"2025-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Budesonide, Added to PTCy-Based Regimen, for Prevention of Acute GI GVHD After Allogeneic Stem Cell Transplantation\",\"authors\":\"Piyanuch Kongtim, Piyatida Chumnumsiriwath, Pongthep Vittayawacharin, Deepa Jeyakumar, Benjamin J. Lee, Jean Doh, Shawn P. Griffin, Richard A. Van Etten, Stefan Ciurea\",\"doi\":\"10.1002/ajh.27581\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Oral budesonide exerts local effects with negligible systemic glucocorticoid activity, due to rapid first-pass metabolism, therefore, could potentially be efficacious in preventing gastrointestinal (GI) acute GVHD (aGVHD). We explored the use of budesonide, added to posttransplant cyclophosphamide (PTCy), tacrolimus, and mycophenolate mofetil, for prevention of GI aGVHD after allogeneic hematopoietic stem cell transplantation (AHSCT) in a prospective observational study and treated 80 patients with a median age of 53 years (range 19–74). Results were compared with a publicly available CIBMTR dataset of 646 patients who received PTCy-based GVHD prophylaxis (CIBMTR Study # GV17-02) (control). Cumulative incidence (CI) of 3-month grade 2–4 and grade 3–4 aGVHD in the budesonide and control groups were 3.8% vs. 34.4% (<i>p</i> < 0.001) and 1.3% vs. 9.8% (<i>p</i> = 0.029), respectively. One-year GRFS (70.5% vs. 31.5%, <i>p</i> < 0.001), PFS (73.4% vs. 52.8%, <i>p</i> = 0.003), and OS (80.1% vs. 64.2%, <i>p</i> = 0.038) were significantly higher in the budesonide group compared with control group. Propensity score-adjusted analyses showed that the addition of budesonide significantly decreased risk of aGVHD grade 2–4 (HR 0.29, <i>p</i> < 0.001), grade 3–4 (HR 0.12, <i>p</i> = 0.045), and cGVHD (HR 0.22, <i>p</i> < 0.001), which resulted in better GRFS (HR 0.38, <i>p</i> < 0.001), PFS (HR 0.58, <i>p</i> = 0.012), and OS (HR 0.72, <i>p</i> = 0.044). Similar results were found when using propensity score-matched analysis restricted to recipients of haploidentical transplantation. In conclusion, addition of budesonide to PTCy-based GVHD prophylaxis is safe and effective in preventing severe acute GI GVHD with significantly improved GRFS. These results could facilitate transition to peripheral blood grafts for all allogeneic transplant recipients.\",\"PeriodicalId\":7724,\"journal\":{\"name\":\"American Journal of Hematology\",\"volume\":\"13 1\",\"pages\":\"\"},\"PeriodicalIF\":10.1000,\"publicationDate\":\"2025-01-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Hematology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ajh.27581\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ajh.27581","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
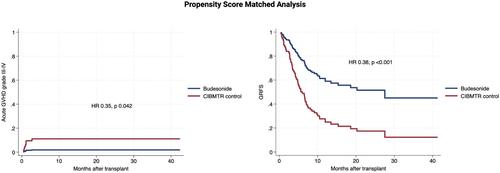
口服布地奈德具有局部作用,全身糖皮质激素活性可忽略不计,由于其快速的首过代谢,因此可能有效预防胃肠道(GI)急性GVHD (aGVHD)。在一项前瞻性观察性研究中,我们探讨了布地奈德与移植后环磷酰胺(PTCy)、他克莫司和霉酚酸酯一起用于预防异基因造血干细胞移植(AHSCT)后GI aGVHD的使用,共治疗了80例患者,中位年龄为53岁(范围19-74岁)。结果与公开的CIBMTR数据集进行了比较,该数据集包括646名接受基于ptc的GVHD预防的患者(CIBMTR Study # GV17-02)(对照组)。布地奈德组和对照组3个月2-4级和3-4级aGVHD累积发生率(CI)分别为3.8% vs. 34.4% (p < 0.001)和1.3% vs. 9.8% (p = 0.029)。布地奈德组1年GRFS (70.5% vs. 31.5%, p < 0.001)、PFS (73.4% vs. 52.8%, p = 0.003)和OS (80.1% vs. 64.2%, p = 0.038)均显著高于对照组。倾向评分调整分析显示,布地奈德的加入显著降低了2-4级aGVHD (HR 0.29, p < 0.001)、3-4级aGVHD (HR 0.12, p = 0.045)和cGVHD (HR 0.22, p < 0.001)的风险,从而改善了GRFS (HR 0.38, p < 0.001)、PFS (HR 0.58, p = 0.012)和OS (HR 0.72, p = 0.044)。当使用倾向评分匹配分析仅限于单倍体移植受者时,发现了类似的结果。综上所述,在基于ptc的GVHD预防中添加布地奈德是安全有效的,可预防严重急性GI GVHD,并显著改善GRFS。这些结果有助于所有同种异体移植受者向外周血移植过渡。
Budesonide, Added to PTCy-Based Regimen, for Prevention of Acute GI GVHD After Allogeneic Stem Cell Transplantation
Oral budesonide exerts local effects with negligible systemic glucocorticoid activity, due to rapid first-pass metabolism, therefore, could potentially be efficacious in preventing gastrointestinal (GI) acute GVHD (aGVHD). We explored the use of budesonide, added to posttransplant cyclophosphamide (PTCy), tacrolimus, and mycophenolate mofetil, for prevention of GI aGVHD after allogeneic hematopoietic stem cell transplantation (AHSCT) in a prospective observational study and treated 80 patients with a median age of 53 years (range 19–74). Results were compared with a publicly available CIBMTR dataset of 646 patients who received PTCy-based GVHD prophylaxis (CIBMTR Study # GV17-02) (control). Cumulative incidence (CI) of 3-month grade 2–4 and grade 3–4 aGVHD in the budesonide and control groups were 3.8% vs. 34.4% (p < 0.001) and 1.3% vs. 9.8% (p = 0.029), respectively. One-year GRFS (70.5% vs. 31.5%, p < 0.001), PFS (73.4% vs. 52.8%, p = 0.003), and OS (80.1% vs. 64.2%, p = 0.038) were significantly higher in the budesonide group compared with control group. Propensity score-adjusted analyses showed that the addition of budesonide significantly decreased risk of aGVHD grade 2–4 (HR 0.29, p < 0.001), grade 3–4 (HR 0.12, p = 0.045), and cGVHD (HR 0.22, p < 0.001), which resulted in better GRFS (HR 0.38, p < 0.001), PFS (HR 0.58, p = 0.012), and OS (HR 0.72, p = 0.044). Similar results were found when using propensity score-matched analysis restricted to recipients of haploidentical transplantation. In conclusion, addition of budesonide to PTCy-based GVHD prophylaxis is safe and effective in preventing severe acute GI GVHD with significantly improved GRFS. These results could facilitate transition to peripheral blood grafts for all allogeneic transplant recipients.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
