{"title":"曲妥珠单抗-帕妥珠单抗联合埃瑞布林或紫杉烷作为治疗人表皮生长因子2阳性局部晚期/转移性乳腺癌的一线化疗:随机非劣效性III期EMERALD试验","authors":"Toshinari Yamashita, Shigehira Saji, Toshimi Takano, Yoichi Naito, Michiko Tsuneizumi, Akiyo Yoshimura, Masato Takahashi, Junji Tsurutani, Tsuguo Iwatani, Masahiro Kitada, Hiroshi Tada, Natsuko Mori, Toru Higuchi, Tsutomu Iwasa, Kazuhiro Araki, Kei Koizumi, Hiroki Hasegawa, Yohei Uchida, Satoshi Morita, Norikazu Masuda","doi":"10.1200/JCO-24-01888","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Trastuzumab-pertuzumab (HP) plus taxane is a current standard first-line therapy for recurrent or metastatic human epidermal growth factor 2 (HER2)+ breast cancer (BC). We investigated noninferiority of eribulin to a taxane when combined with dual HER2 blockade as first-line systemic treatment for locally advanced/metastatic HER2+ BC.</p><p><strong>Methods: </strong>In the phase III EMERALD trial (target sample size, 480; ClinicalTrials.gov identifier: NCT03264547/UMIN000027938), patients were randomly assigned (1:1) to receive eribulin 1.4 mg/m<sup>2</sup> once daily on days 1 and 8 (eribulin group) or a taxane (docetaxel 75 mg/m<sup>2</sup> once on day 1 or paclitaxel 80 mg/m<sup>2</sup> once daily on days 1, 8, and 15; taxane group) intravenously in a 21-day cycle, each with HP on day 1. The primary end point was progression-free survival (PFS; intention-to-treat population). Secondary end points included objective response rate, overall survival (OS), patient-reported quality of life (QoL), and safety. Noninferiority was tested using the stratified Cox proportional hazards model to estimate hazard ratios (HRs) for PFS events, with a noninferiority HR margin of 1.33.</p><p><strong>Results: </strong>Between August 2017 and June 2021, 446 patients (median age, 56.0 years) were enrolled. The median PFS was 14.0 and 12.9 months in the eribulin group (n = 224) and taxane group (n = 222 [docetaxel/paclitaxel, n = 186/36]), respectively (HR, 0.95 [95% CI, 0.76 to 1.19]), which confirmed the noninferiority of the study regimen. The median OS was 65.3 months in the taxane group but has not been reached in the eribulin group. Median time to QoL deterioration was numerically longer with eribulin than with taxane. Adverse event (AE) rates were similar, despite the longer duration of eribulin use. Infusion reaction, skin-related AEs, diarrhea, and edema were more common with taxane, whereas neutropenia was more common with eribulin.</p><p><strong>Conclusion: </strong>The results suggested that eribulin + HP is an option for first-line treatment of locally advanced/metastatic HER2+ BC.</p>","PeriodicalId":15384,"journal":{"name":"Journal of Clinical Oncology","volume":" ","pages":"1302-1313"},"PeriodicalIF":41.9000,"publicationDate":"2025-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11974627/pdf/","citationCount":"0","resultStr":"{\"title\":\"Trastuzumab-Pertuzumab Plus Eribulin or Taxane as First-Line Chemotherapy for Human Epidermal Growth Factor 2-Positive Locally Advanced/Metastatic Breast Cancer: The Randomized Noninferiority Phase III EMERALD Trial.\",\"authors\":\"Toshinari Yamashita, Shigehira Saji, Toshimi Takano, Yoichi Naito, Michiko Tsuneizumi, Akiyo Yoshimura, Masato Takahashi, Junji Tsurutani, Tsuguo Iwatani, Masahiro Kitada, Hiroshi Tada, Natsuko Mori, Toru Higuchi, Tsutomu Iwasa, Kazuhiro Araki, Kei Koizumi, Hiroki Hasegawa, Yohei Uchida, Satoshi Morita, Norikazu Masuda\",\"doi\":\"10.1200/JCO-24-01888\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Trastuzumab-pertuzumab (HP) plus taxane is a current standard first-line therapy for recurrent or metastatic human epidermal growth factor 2 (HER2)+ breast cancer (BC). We investigated noninferiority of eribulin to a taxane when combined with dual HER2 blockade as first-line systemic treatment for locally advanced/metastatic HER2+ BC.</p><p><strong>Methods: </strong>In the phase III EMERALD trial (target sample size, 480; ClinicalTrials.gov identifier: NCT03264547/UMIN000027938), patients were randomly assigned (1:1) to receive eribulin 1.4 mg/m<sup>2</sup> once daily on days 1 and 8 (eribulin group) or a taxane (docetaxel 75 mg/m<sup>2</sup> once on day 1 or paclitaxel 80 mg/m<sup>2</sup> once daily on days 1, 8, and 15; taxane group) intravenously in a 21-day cycle, each with HP on day 1. The primary end point was progression-free survival (PFS; intention-to-treat population). Secondary end points included objective response rate, overall survival (OS), patient-reported quality of life (QoL), and safety. Noninferiority was tested using the stratified Cox proportional hazards model to estimate hazard ratios (HRs) for PFS events, with a noninferiority HR margin of 1.33.</p><p><strong>Results: </strong>Between August 2017 and June 2021, 446 patients (median age, 56.0 years) were enrolled. The median PFS was 14.0 and 12.9 months in the eribulin group (n = 224) and taxane group (n = 222 [docetaxel/paclitaxel, n = 186/36]), respectively (HR, 0.95 [95% CI, 0.76 to 1.19]), which confirmed the noninferiority of the study regimen. The median OS was 65.3 months in the taxane group but has not been reached in the eribulin group. Median time to QoL deterioration was numerically longer with eribulin than with taxane. Adverse event (AE) rates were similar, despite the longer duration of eribulin use. Infusion reaction, skin-related AEs, diarrhea, and edema were more common with taxane, whereas neutropenia was more common with eribulin.</p><p><strong>Conclusion: </strong>The results suggested that eribulin + HP is an option for first-line treatment of locally advanced/metastatic HER2+ BC.</p>\",\"PeriodicalId\":15384,\"journal\":{\"name\":\"Journal of Clinical Oncology\",\"volume\":\" \",\"pages\":\"1302-1313\"},\"PeriodicalIF\":41.9000,\"publicationDate\":\"2025-04-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11974627/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1200/JCO-24-01888\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/9 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1200/JCO-24-01888","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/9 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Trastuzumab-Pertuzumab Plus Eribulin or Taxane as First-Line Chemotherapy for Human Epidermal Growth Factor 2-Positive Locally Advanced/Metastatic Breast Cancer: The Randomized Noninferiority Phase III EMERALD Trial.
Purpose: Trastuzumab-pertuzumab (HP) plus taxane is a current standard first-line therapy for recurrent or metastatic human epidermal growth factor 2 (HER2)+ breast cancer (BC). We investigated noninferiority of eribulin to a taxane when combined with dual HER2 blockade as first-line systemic treatment for locally advanced/metastatic HER2+ BC.
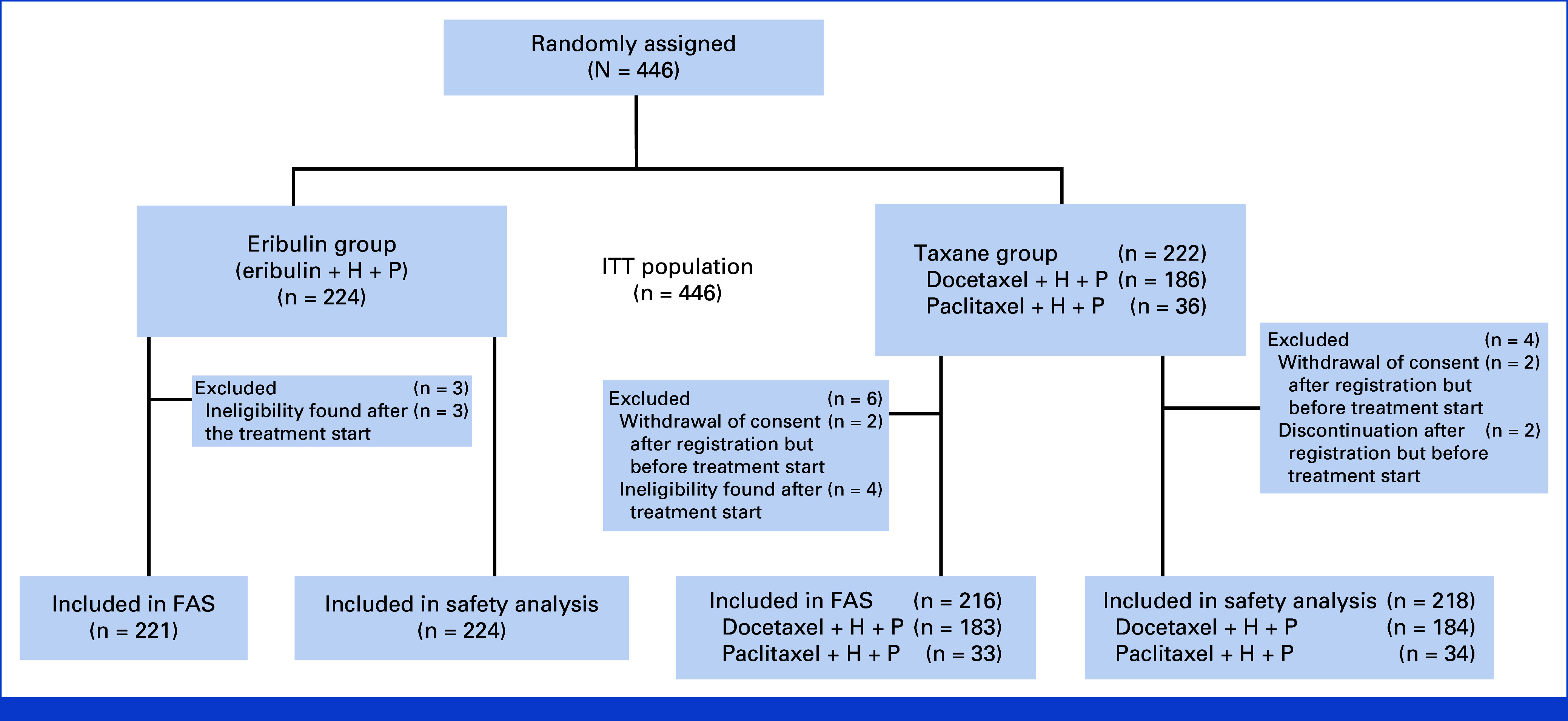
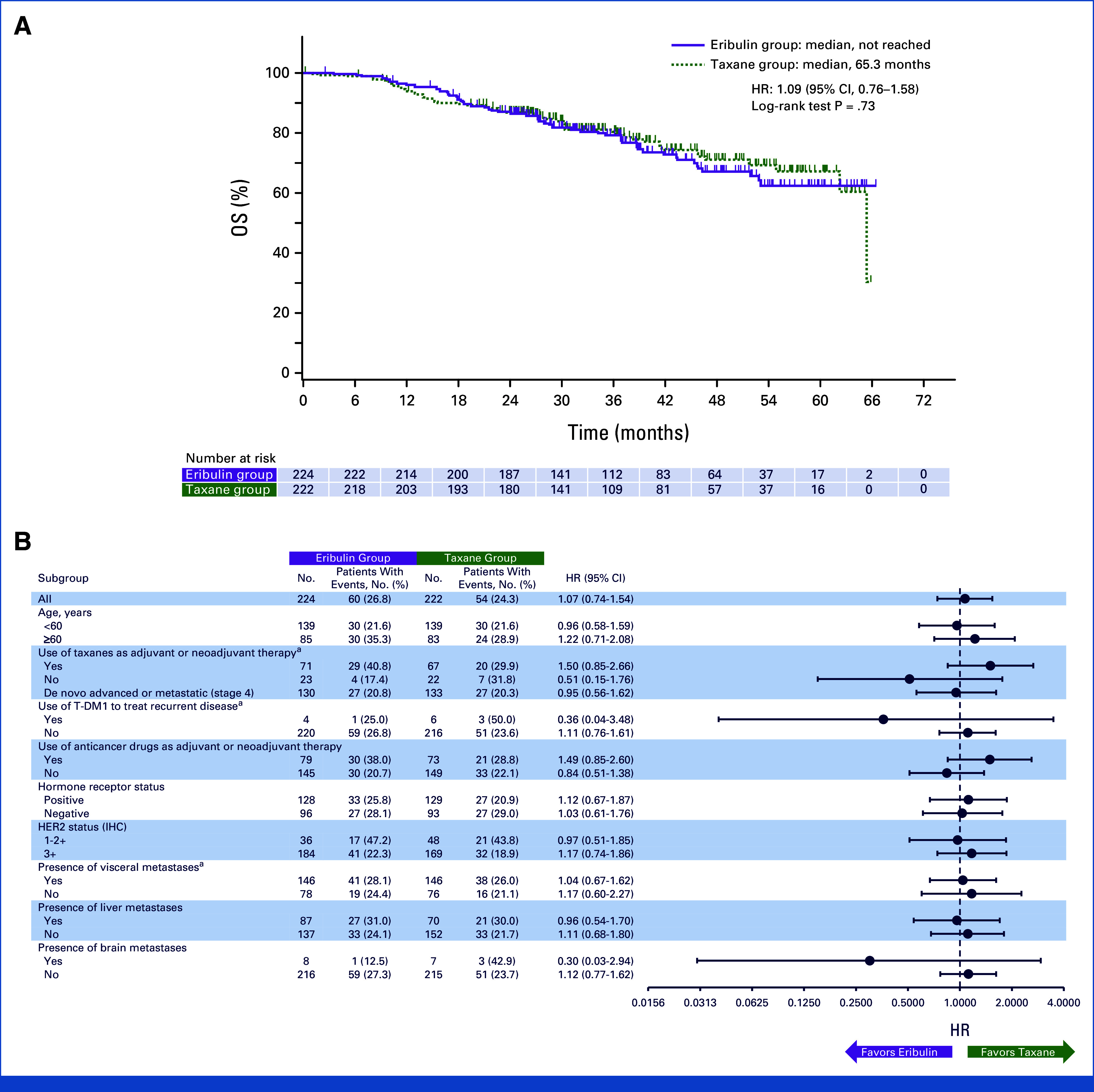
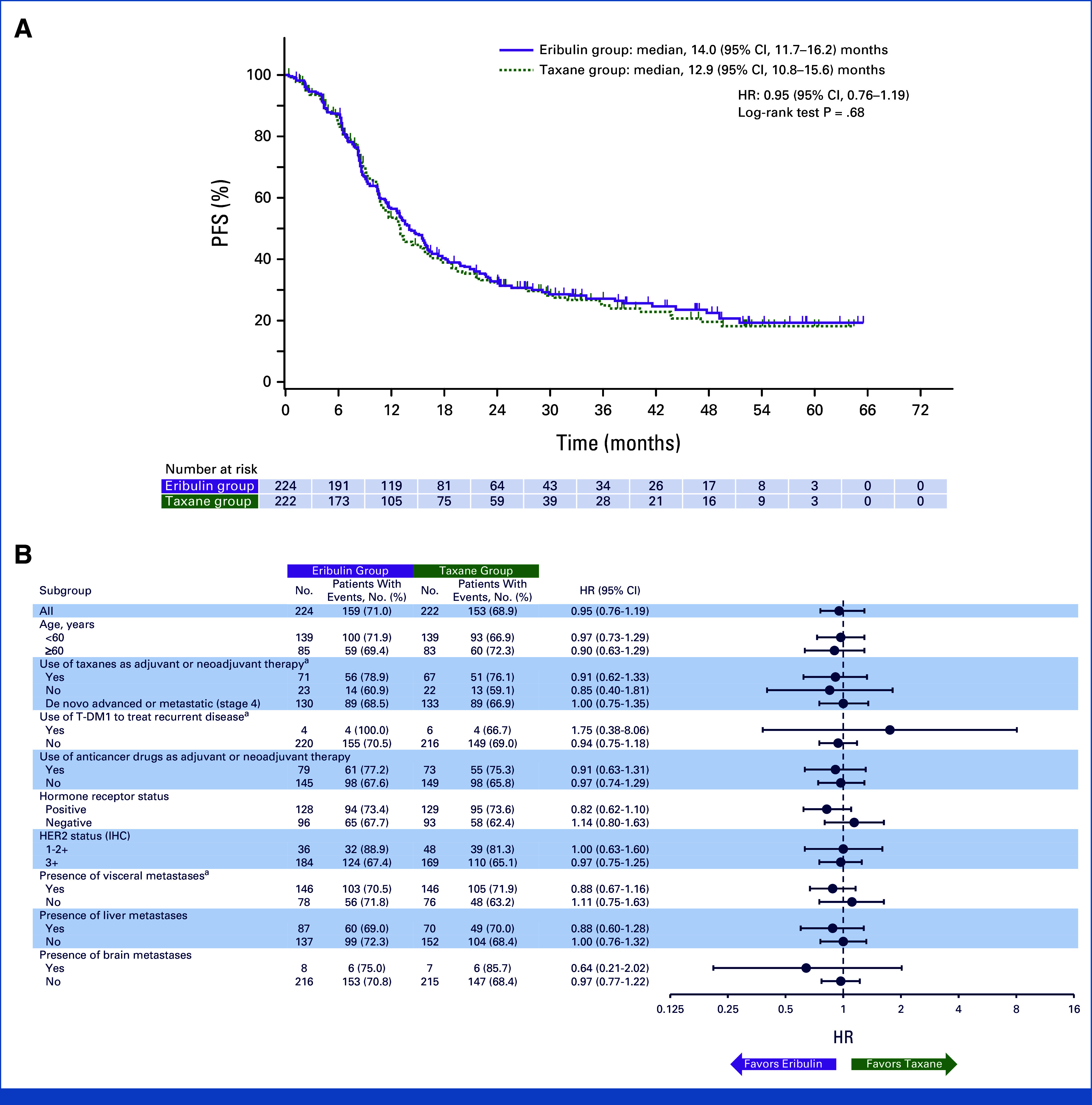
Methods: In the phase III EMERALD trial (target sample size, 480; ClinicalTrials.gov identifier: NCT03264547/UMIN000027938), patients were randomly assigned (1:1) to receive eribulin 1.4 mg/m2 once daily on days 1 and 8 (eribulin group) or a taxane (docetaxel 75 mg/m2 once on day 1 or paclitaxel 80 mg/m2 once daily on days 1, 8, and 15; taxane group) intravenously in a 21-day cycle, each with HP on day 1. The primary end point was progression-free survival (PFS; intention-to-treat population). Secondary end points included objective response rate, overall survival (OS), patient-reported quality of life (QoL), and safety. Noninferiority was tested using the stratified Cox proportional hazards model to estimate hazard ratios (HRs) for PFS events, with a noninferiority HR margin of 1.33.
Results: Between August 2017 and June 2021, 446 patients (median age, 56.0 years) were enrolled. The median PFS was 14.0 and 12.9 months in the eribulin group (n = 224) and taxane group (n = 222 [docetaxel/paclitaxel, n = 186/36]), respectively (HR, 0.95 [95% CI, 0.76 to 1.19]), which confirmed the noninferiority of the study regimen. The median OS was 65.3 months in the taxane group but has not been reached in the eribulin group. Median time to QoL deterioration was numerically longer with eribulin than with taxane. Adverse event (AE) rates were similar, despite the longer duration of eribulin use. Infusion reaction, skin-related AEs, diarrhea, and edema were more common with taxane, whereas neutropenia was more common with eribulin.
Conclusion: The results suggested that eribulin + HP is an option for first-line treatment of locally advanced/metastatic HER2+ BC.
期刊介绍:
The Journal of Clinical Oncology serves its readers as the single most credible, authoritative resource for disseminating significant clinical oncology research. In print and in electronic format, JCO strives to publish the highest quality articles dedicated to clinical research. Original Reports remain the focus of JCO, but this scientific communication is enhanced by appropriately selected Editorials, Commentaries, Reviews, and other work that relate to the care of patients with cancer.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
