Spela Leiler MD , Andre Bauer PhD , Wolfgang Hitzl PhD , Rok Bernik MD , Valentin Guenzler MD , Matthias Angerer MD , Theodor Fischlein PhD , Jurij Matija Kalisnik PhD
{"title":"心房传导阻滞是心脏手术后新发心房颤动的独立危险因素。","authors":"Spela Leiler MD , Andre Bauer PhD , Wolfgang Hitzl PhD , Rok Bernik MD , Valentin Guenzler MD , Matthias Angerer MD , Theodor Fischlein PhD , Jurij Matija Kalisnik PhD","doi":"10.1016/j.xjon.2024.10.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>This study aims to investigate the association between interatrial conduction block and postoperative atrial fibrillation, which can precipitate acute cardiopulmonary instability and is associated with subsequent heart failure, stroke, and mortality following cardiac surgery.</div></div><div><h3>Methods</h3><div>Perioperative 12-channel electrocardiograms from 3405 patients undergoing myocardial revascularization, valve surgery, aortic surgery, or combinations thereof, were considered. Clinical and electrographic parameters were compared between patients with and without atrial fibrillation, and significant variables were analyzed using univariate and multivariate logistic regression.</div></div><div><h3>Results</h3><div>Among 2108 analyzed patients, 764 (36.2%) developed atrial fibrillation. Preoperative interatrial block was a strong independent risk factor (3.18; 95% CI, 2.55, 3.96; <em>P</em> < .001), significantly improving area under the receiver operator characteristics curve from 71.8% to 75.6% (Delong's test: <em>P</em> = .013). Other risk factors included advanced age (1.05; 95% CI, 1.03, 1.07; <em>P</em> < .001), female gender (1.86; 95% CI, 1.45, 2.38; <em>P</em> < .001), history of cardiogenic shock (1.44; 95% CI, 0.99, 2.09; <em>P</em> = .057), reduced left ventricular ejection fraction <40% (1.57; 95% CI, 1.06, 2.33; <em>P</em> = .024), cessation of preoperative β-blockers (1.17; 95% CI, 0.95, 1.46; <em>P</em> = .145), score for clinical prediction rules for estimating the risk of stroke in people with non-rheumatic atrial fibrillation (CHAS<sub>2</sub>DS<sub>2</sub>-VASc) and European System for Cardiac Operative Risk Evaluation II score (0.87; 95% CI, 0.79, 0.97; <em>P</em> = .01) and (1.04; 95% CI, 0.99, 1.11; <em>P</em> = .138), preexisting left bundle branch block (1.59; 95% CI, 0.92, 2.74; <em>P</em> = .097), cardiopulmonary bypass time (1.00; 95% CI, 1.00, 1.00; <em>P</em> = .049), bicaval cannulation (1.45; 95% CI, 0.88, 2.41; <em>P</em> = .035), cardiac surgery-associated acute kidney injury (3.19; 95% CI, 2.45, 4.15; <em>P</em> < .001), and postoperative atrioventricular block (1.20; 95% CI, 0.96, 1.51; <em>P</em> = .105), particularly Mobitz I (6.73; 95% CI, 1.98, 31.51; <em>P</em> = .005).</div></div><div><h3>Conclusions</h3><div>Perioperative electrocardiogram-derived parameters, especially interatrial block, are associated with postoperative atrial fibrillation. Further research is needed to clarify the link between conduction abnormalities and postoperative atrial fibrillation, enabling targeted prophylactic therapies for high-risk patients.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"22 ","pages":"Pages 345-353"},"PeriodicalIF":1.9000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704582/pdf/","citationCount":"0","resultStr":"{\"title\":\"Interatrial block is an independent risk factor for new-onset atrial fibrillation after cardiac surgery\",\"authors\":\"Spela Leiler MD , Andre Bauer PhD , Wolfgang Hitzl PhD , Rok Bernik MD , Valentin Guenzler MD , Matthias Angerer MD , Theodor Fischlein PhD , Jurij Matija Kalisnik PhD\",\"doi\":\"10.1016/j.xjon.2024.10.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objectives</h3><div>This study aims to investigate the association between interatrial conduction block and postoperative atrial fibrillation, which can precipitate acute cardiopulmonary instability and is associated with subsequent heart failure, stroke, and mortality following cardiac surgery.</div></div><div><h3>Methods</h3><div>Perioperative 12-channel electrocardiograms from 3405 patients undergoing myocardial revascularization, valve surgery, aortic surgery, or combinations thereof, were considered. Clinical and electrographic parameters were compared between patients with and without atrial fibrillation, and significant variables were analyzed using univariate and multivariate logistic regression.</div></div><div><h3>Results</h3><div>Among 2108 analyzed patients, 764 (36.2%) developed atrial fibrillation. Preoperative interatrial block was a strong independent risk factor (3.18; 95% CI, 2.55, 3.96; <em>P</em> < .001), significantly improving area under the receiver operator characteristics curve from 71.8% to 75.6% (Delong's test: <em>P</em> = .013). Other risk factors included advanced age (1.05; 95% CI, 1.03, 1.07; <em>P</em> < .001), female gender (1.86; 95% CI, 1.45, 2.38; <em>P</em> < .001), history of cardiogenic shock (1.44; 95% CI, 0.99, 2.09; <em>P</em> = .057), reduced left ventricular ejection fraction <40% (1.57; 95% CI, 1.06, 2.33; <em>P</em> = .024), cessation of preoperative β-blockers (1.17; 95% CI, 0.95, 1.46; <em>P</em> = .145), score for clinical prediction rules for estimating the risk of stroke in people with non-rheumatic atrial fibrillation (CHAS<sub>2</sub>DS<sub>2</sub>-VASc) and European System for Cardiac Operative Risk Evaluation II score (0.87; 95% CI, 0.79, 0.97; <em>P</em> = .01) and (1.04; 95% CI, 0.99, 1.11; <em>P</em> = .138), preexisting left bundle branch block (1.59; 95% CI, 0.92, 2.74; <em>P</em> = .097), cardiopulmonary bypass time (1.00; 95% CI, 1.00, 1.00; <em>P</em> = .049), bicaval cannulation (1.45; 95% CI, 0.88, 2.41; <em>P</em> = .035), cardiac surgery-associated acute kidney injury (3.19; 95% CI, 2.45, 4.15; <em>P</em> < .001), and postoperative atrioventricular block (1.20; 95% CI, 0.96, 1.51; <em>P</em> = .105), particularly Mobitz I (6.73; 95% CI, 1.98, 31.51; <em>P</em> = .005).</div></div><div><h3>Conclusions</h3><div>Perioperative electrocardiogram-derived parameters, especially interatrial block, are associated with postoperative atrial fibrillation. Further research is needed to clarify the link between conduction abnormalities and postoperative atrial fibrillation, enabling targeted prophylactic therapies for high-risk patients.</div></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"22 \",\"pages\":\"Pages 345-353\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704582/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666273624002778\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273624002778","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
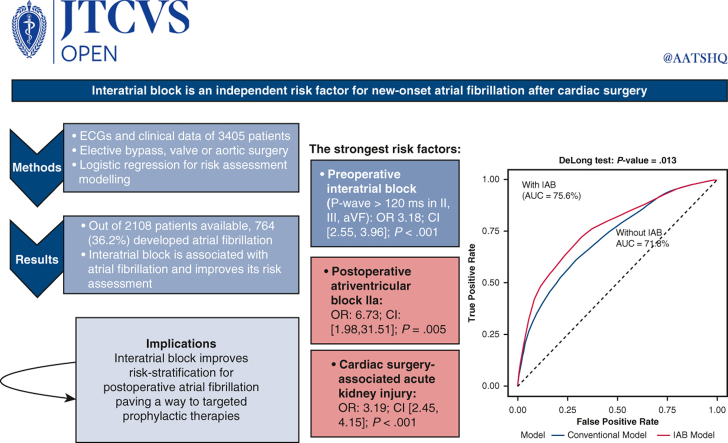
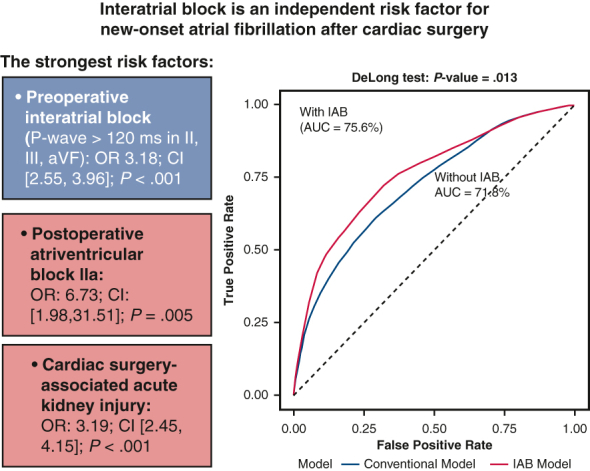
Interatrial block is an independent risk factor for new-onset atrial fibrillation after cardiac surgery
Objectives
This study aims to investigate the association between interatrial conduction block and postoperative atrial fibrillation, which can precipitate acute cardiopulmonary instability and is associated with subsequent heart failure, stroke, and mortality following cardiac surgery.
Methods
Perioperative 12-channel electrocardiograms from 3405 patients undergoing myocardial revascularization, valve surgery, aortic surgery, or combinations thereof, were considered. Clinical and electrographic parameters were compared between patients with and without atrial fibrillation, and significant variables were analyzed using univariate and multivariate logistic regression.
Results
Among 2108 analyzed patients, 764 (36.2%) developed atrial fibrillation. Preoperative interatrial block was a strong independent risk factor (3.18; 95% CI, 2.55, 3.96; P < .001), significantly improving area under the receiver operator characteristics curve from 71.8% to 75.6% (Delong's test: P = .013). Other risk factors included advanced age (1.05; 95% CI, 1.03, 1.07; P < .001), female gender (1.86; 95% CI, 1.45, 2.38; P < .001), history of cardiogenic shock (1.44; 95% CI, 0.99, 2.09; P = .057), reduced left ventricular ejection fraction <40% (1.57; 95% CI, 1.06, 2.33; P = .024), cessation of preoperative β-blockers (1.17; 95% CI, 0.95, 1.46; P = .145), score for clinical prediction rules for estimating the risk of stroke in people with non-rheumatic atrial fibrillation (CHAS2DS2-VASc) and European System for Cardiac Operative Risk Evaluation II score (0.87; 95% CI, 0.79, 0.97; P = .01) and (1.04; 95% CI, 0.99, 1.11; P = .138), preexisting left bundle branch block (1.59; 95% CI, 0.92, 2.74; P = .097), cardiopulmonary bypass time (1.00; 95% CI, 1.00, 1.00; P = .049), bicaval cannulation (1.45; 95% CI, 0.88, 2.41; P = .035), cardiac surgery-associated acute kidney injury (3.19; 95% CI, 2.45, 4.15; P < .001), and postoperative atrioventricular block (1.20; 95% CI, 0.96, 1.51; P = .105), particularly Mobitz I (6.73; 95% CI, 1.98, 31.51; P = .005).
Conclusions
Perioperative electrocardiogram-derived parameters, especially interatrial block, are associated with postoperative atrial fibrillation. Further research is needed to clarify the link between conduction abnormalities and postoperative atrial fibrillation, enabling targeted prophylactic therapies for high-risk patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
