Madison T Taychert, Shane A Wells, Jordan R Krieger, Ethan Richmond, Glenn O Allen, Emily Serrell, Ali S Antar, Margaret A Knoedler, Christopher M Manakas, Dan R Gralnek, Matthew D Grimes
{"title":"mri衍生的过渡区指数可高度预测钬激光前列腺摘除前尿动力性膀胱出口梗阻。","authors":"Madison T Taychert, Shane A Wells, Jordan R Krieger, Ethan Richmond, Glenn O Allen, Emily Serrell, Ali S Antar, Margaret A Knoedler, Christopher M Manakas, Dan R Gralnek, Matthew D Grimes","doi":"10.1002/nau.25660","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and objective: </strong>Urodynamic study (UDS) is required to diagnose bladder outlet obstruction (BOO) during evaluation of benign prostatic hyperplasia (BPH) but is seldom performed due to cost and invasiveness. Therefore, anatomic and clinical parameters to predict BOO have been proposed, including the prostate transition zone index (TZI) which is the ratio of prostate transition zone volume (TZV) to whole gland volume (WGV). Historically computed with ellipsoid volume estimation of prostate WGV and TZV from transrectal ultrasound measurements, controversy exists regarding the utility of TZI to predict likelihood of BOO on UDS and clinical outcomes following BPH surgery. Here, we aim to assess the association between MRI-measured TZI and BOO on preoperative UDS in a modern BPH cohort before holmium laser enucleation of the prostate (HoLEP).</p><p><strong>Methods: </strong>A prospectively maintained institutional database of 944 consecutive HoLEP patients between 2018 and 2022 was reviewed to identify those with preoperative UDS and MRI within 1 year of surgery. UDS was used to measure bladder outlet obstruction index (BOOI). 3D WGV and TZV were estimated using clinically available software (DynaCAD). We used linear regression to assess the relationship between TZI, WGV, and BOOI and logistic regression to determine the association between TZI, WGV, and BOO (defined as BOOI > 40).</p><p><strong>Results: </strong>45/944 (4.8%) patients had both preoperative UDS and MRI within 1 year of HoLEP. Of these, 27 patients were obstructed (BOOI > 40) and 18 patients were not obstructed (BOOI ≤ 40) on preoperative UDS. Obstructed patients had larger prostate WGV, TZV, and TZI compared to non-obstructed patients but were otherwise similar with respect to preoperative characteristics. Univariate analysis showed a positive association between TZI and BOO (R<sup>2</sup> = 0.373, p < 0.001) and WGV and BOO (R<sup>2</sup> = 0.214, p < 0.001). Multivariable logistic regression showed that TZI was independently associated with BOO (OR 1.08, 95% CI 1.02-1.14, p = 0.013) while accounting for WGV. WGV was not independently associated with BOO while accounting for TZI (OR 1.00, 95% CI 0.98-1.01, p = 0.614). The Youden index was utilized to create an optimal cutpoint for TZI (0.528) above which urodynamic BOO was very likely on multivariate logistic regression while accounting for WGV (OR 25.0, 95% CI 3.40-183.58, p = 0.002). The generated cutpoint for WGV (61.5 mL) was not significantly associated with urodynamic BOO on multivariate logistic regression while accounting for TZI (OR 0.993, 95% CI 0.98-1.01, p = 0.452).</p><p><strong>Conclusions: </strong>Noninvasive MRI measurement of prostate TZI was highly and independently predictive of BOO before HoLEP and superior to WGV alone. This suggests that MRI obtained in evaluation of BPH/LUTS patients may be used to calculate TZI and inform patient selection for invasive urodynamic study and surgical treatment.</p>","PeriodicalId":19200,"journal":{"name":"Neurourology and Urodynamics","volume":" ","pages":"367-373"},"PeriodicalIF":2.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11788939/pdf/","citationCount":"0","resultStr":"{\"title\":\"MRI-Derived Transition Zone Index Is Highly Predictive of Urodynamic Bladder Outlet Obstruction Prior to Holmium Laser Enucleation of the Prostate.\",\"authors\":\"Madison T Taychert, Shane A Wells, Jordan R Krieger, Ethan Richmond, Glenn O Allen, Emily Serrell, Ali S Antar, Margaret A Knoedler, Christopher M Manakas, Dan R Gralnek, Matthew D Grimes\",\"doi\":\"10.1002/nau.25660\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction and objective: </strong>Urodynamic study (UDS) is required to diagnose bladder outlet obstruction (BOO) during evaluation of benign prostatic hyperplasia (BPH) but is seldom performed due to cost and invasiveness. Therefore, anatomic and clinical parameters to predict BOO have been proposed, including the prostate transition zone index (TZI) which is the ratio of prostate transition zone volume (TZV) to whole gland volume (WGV). Historically computed with ellipsoid volume estimation of prostate WGV and TZV from transrectal ultrasound measurements, controversy exists regarding the utility of TZI to predict likelihood of BOO on UDS and clinical outcomes following BPH surgery. Here, we aim to assess the association between MRI-measured TZI and BOO on preoperative UDS in a modern BPH cohort before holmium laser enucleation of the prostate (HoLEP).</p><p><strong>Methods: </strong>A prospectively maintained institutional database of 944 consecutive HoLEP patients between 2018 and 2022 was reviewed to identify those with preoperative UDS and MRI within 1 year of surgery. UDS was used to measure bladder outlet obstruction index (BOOI). 3D WGV and TZV were estimated using clinically available software (DynaCAD). We used linear regression to assess the relationship between TZI, WGV, and BOOI and logistic regression to determine the association between TZI, WGV, and BOO (defined as BOOI > 40).</p><p><strong>Results: </strong>45/944 (4.8%) patients had both preoperative UDS and MRI within 1 year of HoLEP. Of these, 27 patients were obstructed (BOOI > 40) and 18 patients were not obstructed (BOOI ≤ 40) on preoperative UDS. Obstructed patients had larger prostate WGV, TZV, and TZI compared to non-obstructed patients but were otherwise similar with respect to preoperative characteristics. Univariate analysis showed a positive association between TZI and BOO (R<sup>2</sup> = 0.373, p < 0.001) and WGV and BOO (R<sup>2</sup> = 0.214, p < 0.001). Multivariable logistic regression showed that TZI was independently associated with BOO (OR 1.08, 95% CI 1.02-1.14, p = 0.013) while accounting for WGV. WGV was not independently associated with BOO while accounting for TZI (OR 1.00, 95% CI 0.98-1.01, p = 0.614). The Youden index was utilized to create an optimal cutpoint for TZI (0.528) above which urodynamic BOO was very likely on multivariate logistic regression while accounting for WGV (OR 25.0, 95% CI 3.40-183.58, p = 0.002). The generated cutpoint for WGV (61.5 mL) was not significantly associated with urodynamic BOO on multivariate logistic regression while accounting for TZI (OR 0.993, 95% CI 0.98-1.01, p = 0.452).</p><p><strong>Conclusions: </strong>Noninvasive MRI measurement of prostate TZI was highly and independently predictive of BOO before HoLEP and superior to WGV alone. This suggests that MRI obtained in evaluation of BPH/LUTS patients may be used to calculate TZI and inform patient selection for invasive urodynamic study and surgical treatment.</p>\",\"PeriodicalId\":19200,\"journal\":{\"name\":\"Neurourology and Urodynamics\",\"volume\":\" \",\"pages\":\"367-373\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11788939/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurourology and Urodynamics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/nau.25660\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurourology and Urodynamics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/nau.25660","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
简介与目的:在评估良性前列腺增生(BPH)时,需要尿动力学研究(UDS)来诊断膀胱出口梗阻(BOO),但由于成本和侵入性,很少进行尿动力学研究。因此,提出了预测BOO的解剖学和临床参数,包括前列腺过渡区指数(TZI),即前列腺过渡区体积(TZV)与整个腺体体积(WGV)的比值。历来通过经直肠超声测量的前列腺WGV和TZV的椭球体积估计来计算,关于TZI在预测UDS上BOO可能性和BPH手术后临床结果方面的应用存在争议。在这里,我们的目的是评估mri测量的TZI和BOO在现代BPH队列术前UDS的相关性钬激光前列腺摘除(HoLEP)之前。方法:回顾2018年至2022年期间944例连续HoLEP患者的前瞻性机构数据库,以确定术前UDS和手术1年内MRI的患者。膀胱出口梗阻指数(BOOI)采用UDS测定。使用临床可用的软件(DynaCAD)估计三维WGV和TZV。我们使用线性回归来评估TZI、WGV和BOOI之间的关系,并使用逻辑回归来确定TZI、WGV和BOO之间的关系(定义为BOOI bbb40)。结果:45/944例(4.8%)患者在HoLEP术后1年内同时行术前UDS和MRI检查。其中术前UDS阻塞27例(BOOI≤40),未阻塞18例(BOOI≤40)。与未梗阻患者相比,梗阻患者的前列腺WGV、TZV和TZI较大,但在术前特征方面其他方面相似。单因素分析显示TZI与BOO呈正相关(R2 = 0.373, p 2 = 0.214, p)。结论:无创MRI测量前列腺TZI对HoLEP前BOO的预测具有高度和独立的意义,优于单纯的WGV。这表明,在评估BPH/LUTS患者时获得的MRI可用于计算TZI,并为患者选择有创尿动力学研究和手术治疗提供信息。
MRI-Derived Transition Zone Index Is Highly Predictive of Urodynamic Bladder Outlet Obstruction Prior to Holmium Laser Enucleation of the Prostate.
Introduction and objective: Urodynamic study (UDS) is required to diagnose bladder outlet obstruction (BOO) during evaluation of benign prostatic hyperplasia (BPH) but is seldom performed due to cost and invasiveness. Therefore, anatomic and clinical parameters to predict BOO have been proposed, including the prostate transition zone index (TZI) which is the ratio of prostate transition zone volume (TZV) to whole gland volume (WGV). Historically computed with ellipsoid volume estimation of prostate WGV and TZV from transrectal ultrasound measurements, controversy exists regarding the utility of TZI to predict likelihood of BOO on UDS and clinical outcomes following BPH surgery. Here, we aim to assess the association between MRI-measured TZI and BOO on preoperative UDS in a modern BPH cohort before holmium laser enucleation of the prostate (HoLEP).
Methods: A prospectively maintained institutional database of 944 consecutive HoLEP patients between 2018 and 2022 was reviewed to identify those with preoperative UDS and MRI within 1 year of surgery. UDS was used to measure bladder outlet obstruction index (BOOI). 3D WGV and TZV were estimated using clinically available software (DynaCAD). We used linear regression to assess the relationship between TZI, WGV, and BOOI and logistic regression to determine the association between TZI, WGV, and BOO (defined as BOOI > 40).
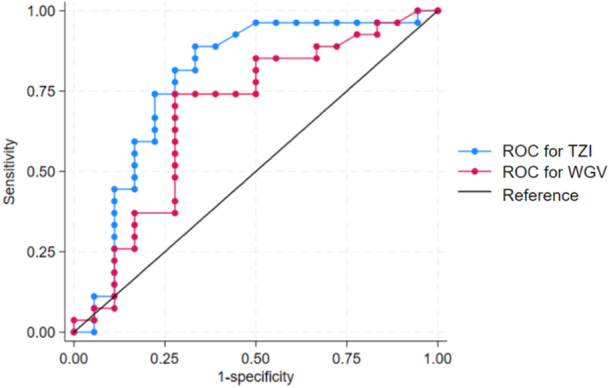
Results: 45/944 (4.8%) patients had both preoperative UDS and MRI within 1 year of HoLEP. Of these, 27 patients were obstructed (BOOI > 40) and 18 patients were not obstructed (BOOI ≤ 40) on preoperative UDS. Obstructed patients had larger prostate WGV, TZV, and TZI compared to non-obstructed patients but were otherwise similar with respect to preoperative characteristics. Univariate analysis showed a positive association between TZI and BOO (R2 = 0.373, p < 0.001) and WGV and BOO (R2 = 0.214, p < 0.001). Multivariable logistic regression showed that TZI was independently associated with BOO (OR 1.08, 95% CI 1.02-1.14, p = 0.013) while accounting for WGV. WGV was not independently associated with BOO while accounting for TZI (OR 1.00, 95% CI 0.98-1.01, p = 0.614). The Youden index was utilized to create an optimal cutpoint for TZI (0.528) above which urodynamic BOO was very likely on multivariate logistic regression while accounting for WGV (OR 25.0, 95% CI 3.40-183.58, p = 0.002). The generated cutpoint for WGV (61.5 mL) was not significantly associated with urodynamic BOO on multivariate logistic regression while accounting for TZI (OR 0.993, 95% CI 0.98-1.01, p = 0.452).
Conclusions: Noninvasive MRI measurement of prostate TZI was highly and independently predictive of BOO before HoLEP and superior to WGV alone. This suggests that MRI obtained in evaluation of BPH/LUTS patients may be used to calculate TZI and inform patient selection for invasive urodynamic study and surgical treatment.
期刊介绍:
Neurourology and Urodynamics welcomes original scientific contributions from all parts of the world on topics related to urinary tract function, urinary and fecal continence and pelvic floor function.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
