Philippe Moreau, Thierry Facon, Saad Z. Usmani, Nizar Bahlis, Noopur Raje, Torben Plesner, Robert Z. Orlowski, Supratik Basu, Hareth Nahi, Cyrille Hulin, Hang Quach, Hartmut Goldschmidt, Michael O’Dwyer, Aurore Perrot, Christopher P. Venner, Katja Weisel, Mourad Tiab, Margaret Macro, Laurent Frenzel, Xavier Leleu, George Wang, Huiling Pei, Maria Krevvata, Robin Carson, Fredrik Borgsten, Shaji K. Kumar
{"title":"达拉单抗联合来那度胺/地塞米松治疗未经治疗的多发性骨髓瘤:MAIA研究的关键亚组分析","authors":"Philippe Moreau, Thierry Facon, Saad Z. Usmani, Nizar Bahlis, Noopur Raje, Torben Plesner, Robert Z. Orlowski, Supratik Basu, Hareth Nahi, Cyrille Hulin, Hang Quach, Hartmut Goldschmidt, Michael O’Dwyer, Aurore Perrot, Christopher P. Venner, Katja Weisel, Mourad Tiab, Margaret Macro, Laurent Frenzel, Xavier Leleu, George Wang, Huiling Pei, Maria Krevvata, Robin Carson, Fredrik Borgsten, Shaji K. Kumar","doi":"10.1038/s41375-024-02506-1","DOIUrl":null,"url":null,"abstract":"In the MAIA study (median follow-up, 56.2 months), daratumumab plus lenalidomide and dexamethasone (D-Rd) significantly improved progression-free survival (PFS) and overall survival versus lenalidomide and dexamethasone (Rd) alone in transplant-ineligible newly diagnosed multiple myeloma (NDMM). In this post hoc analysis of clinically important subgroups in MAIA (median follow-up, 64.5 months), transplant-ineligible patients with NDMM were randomized 1:1 to D-Rd or Rd. The primary endpoint was PFS; secondary endpoints included overall response rate (ORR) and measurable residual disease (MRD)–negativity rate (10–5). PFS favored D-Rd versus Rd in most subgroups, including patients aged ≥75 years (HR, 0.59; 95% CI, 0.44–0.79), frail patients (HR, 0.64; 95% CI, 0.48–0.85), patients with high-risk cytogenetics (HR, 0.59; 95% CI, 0.44–0.80), and patients with isolated gain(1q21) (HR, 0.36; 95% CI, 0.19–0.67). ORRs, MRD-negativity rates, and sustained (≥12 months) MRD-negativity rates were higher with D-Rd versus Rd across subgroups. In patients aged ≥75 years, rates of grade 3/4 and serious treatment-emergent adverse events (TEAEs) were similar for D-Rd and Rd, but discontinuation due to TEAEs was lower for D-Rd. Results support use of D-Rd for high-risk patients, supporting D-Rd as a standard of care for transplant-ineligible NDMM. This trial was registered at www.clinicaltrials.gov as NCT02252172.","PeriodicalId":18109,"journal":{"name":"Leukemia","volume":"39 3","pages":"710-719"},"PeriodicalIF":8.8000,"publicationDate":"2025-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Daratumumab plus lenalidomide/dexamethasone in untreated multiple myeloma: analysis of key subgroups of the MAIA study\",\"authors\":\"Philippe Moreau, Thierry Facon, Saad Z. Usmani, Nizar Bahlis, Noopur Raje, Torben Plesner, Robert Z. Orlowski, Supratik Basu, Hareth Nahi, Cyrille Hulin, Hang Quach, Hartmut Goldschmidt, Michael O’Dwyer, Aurore Perrot, Christopher P. Venner, Katja Weisel, Mourad Tiab, Margaret Macro, Laurent Frenzel, Xavier Leleu, George Wang, Huiling Pei, Maria Krevvata, Robin Carson, Fredrik Borgsten, Shaji K. Kumar\",\"doi\":\"10.1038/s41375-024-02506-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"In the MAIA study (median follow-up, 56.2 months), daratumumab plus lenalidomide and dexamethasone (D-Rd) significantly improved progression-free survival (PFS) and overall survival versus lenalidomide and dexamethasone (Rd) alone in transplant-ineligible newly diagnosed multiple myeloma (NDMM). In this post hoc analysis of clinically important subgroups in MAIA (median follow-up, 64.5 months), transplant-ineligible patients with NDMM were randomized 1:1 to D-Rd or Rd. The primary endpoint was PFS; secondary endpoints included overall response rate (ORR) and measurable residual disease (MRD)–negativity rate (10–5). PFS favored D-Rd versus Rd in most subgroups, including patients aged ≥75 years (HR, 0.59; 95% CI, 0.44–0.79), frail patients (HR, 0.64; 95% CI, 0.48–0.85), patients with high-risk cytogenetics (HR, 0.59; 95% CI, 0.44–0.80), and patients with isolated gain(1q21) (HR, 0.36; 95% CI, 0.19–0.67). ORRs, MRD-negativity rates, and sustained (≥12 months) MRD-negativity rates were higher with D-Rd versus Rd across subgroups. In patients aged ≥75 years, rates of grade 3/4 and serious treatment-emergent adverse events (TEAEs) were similar for D-Rd and Rd, but discontinuation due to TEAEs was lower for D-Rd. Results support use of D-Rd for high-risk patients, supporting D-Rd as a standard of care for transplant-ineligible NDMM. This trial was registered at www.clinicaltrials.gov as NCT02252172.\",\"PeriodicalId\":18109,\"journal\":{\"name\":\"Leukemia\",\"volume\":\"39 3\",\"pages\":\"710-719\"},\"PeriodicalIF\":8.8000,\"publicationDate\":\"2025-01-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Leukemia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.nature.com/articles/s41375-024-02506-1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Leukemia","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41375-024-02506-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
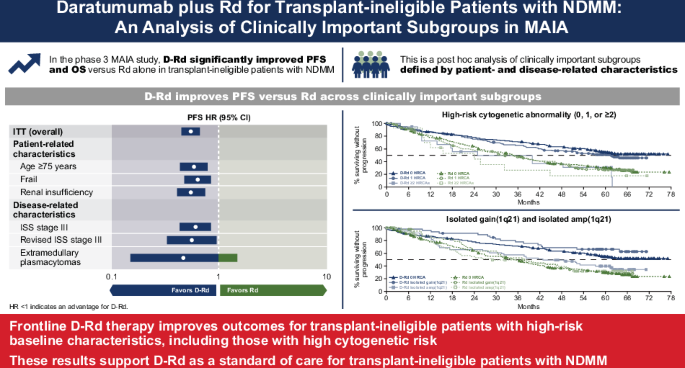
Daratumumab plus lenalidomide/dexamethasone in untreated multiple myeloma: analysis of key subgroups of the MAIA study
In the MAIA study (median follow-up, 56.2 months), daratumumab plus lenalidomide and dexamethasone (D-Rd) significantly improved progression-free survival (PFS) and overall survival versus lenalidomide and dexamethasone (Rd) alone in transplant-ineligible newly diagnosed multiple myeloma (NDMM). In this post hoc analysis of clinically important subgroups in MAIA (median follow-up, 64.5 months), transplant-ineligible patients with NDMM were randomized 1:1 to D-Rd or Rd. The primary endpoint was PFS; secondary endpoints included overall response rate (ORR) and measurable residual disease (MRD)–negativity rate (10–5). PFS favored D-Rd versus Rd in most subgroups, including patients aged ≥75 years (HR, 0.59; 95% CI, 0.44–0.79), frail patients (HR, 0.64; 95% CI, 0.48–0.85), patients with high-risk cytogenetics (HR, 0.59; 95% CI, 0.44–0.80), and patients with isolated gain(1q21) (HR, 0.36; 95% CI, 0.19–0.67). ORRs, MRD-negativity rates, and sustained (≥12 months) MRD-negativity rates were higher with D-Rd versus Rd across subgroups. In patients aged ≥75 years, rates of grade 3/4 and serious treatment-emergent adverse events (TEAEs) were similar for D-Rd and Rd, but discontinuation due to TEAEs was lower for D-Rd. Results support use of D-Rd for high-risk patients, supporting D-Rd as a standard of care for transplant-ineligible NDMM. This trial was registered at www.clinicaltrials.gov as NCT02252172.
期刊介绍:
Title: Leukemia
Journal Overview:
Publishes high-quality, peer-reviewed research
Covers all aspects of research and treatment of leukemia and allied diseases
Includes studies of normal hemopoiesis due to comparative relevance
Topics of Interest:
Oncogenes
Growth factors
Stem cells
Leukemia genomics
Cell cycle
Signal transduction
Molecular targets for therapy
And more
Content Types:
Original research articles
Reviews
Letters
Correspondence
Comments elaborating on significant advances and covering topical issues





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
